Whether you're a patient scheduled for your first procedure, a clinician reviewing current standards, or a healthcare procurement officer evaluating equipment performance, this article covers what matters: how the procedure works, how to prepare effectively, how to interpret results, and why equipment quality directly influences diagnostic accuracy.
Key Takeaways
- Video colonoscopes use a digital CCD or CMOS sensor — not fiber-optic glass bundles — delivering real-time high-definition imaging to an external monitor
- Bowel preparation quality is the single most patient-controllable factor; poor prep is linked to a 42% adenoma miss rate (per published gastroenterology literature)
- Scope insertion and examination typically takes 30–60 minutes under conscious sedation
- Results arrive in two phases: physicians report immediate visual findings on-site, while biopsy lab results take days and vary by facility
- Equipment generation matters — newer wide-angle HD colonoscopes have demonstrated a 22% higher adenoma detection rate than mixed older-technology units (based on comparative endoscopy studies)
What Is a Video Colonoscope?
A video colonoscope is a flexible lower-gastrointestinal endoscope designed for large-bowel examination. The "video" designation refers to a solid-state digital sensor at the distal tip — either a CCD (Olympus 190-series) or CMOS (Fujifilm ELUXEO 800 series) — that transmits live images to an external monitor. This sets it apart from older fiber-optic colonoscopes, which relay images through bundled glass fibers at lower resolution.
Key Components
| Component | Function |
|---|---|
| Control head | Houses suction, insufflation, and angulation knobs |
| Insertion tube | Approximately 133–169 cm depending on model |
| Distal tip | Camera, light source, and irrigation port |
| Working channel | Passes biopsy forceps, snares, and clip devices |
Video colonoscopy and virtual colonoscopy are distinct procedures. Virtual colonoscopy (CT colonography) uses X-ray imaging to generate a 3D map of the colon without scope insertion — but it cannot remove polyps or take biopsies. Any suspicious finding still requires a follow-up standard colonoscopy.
Why Video Colonoscopy Is Used
The procedure combines detection, biopsy, and treatment in a single session. No other colorectal screening tool delivers all three capabilities at once.
Primary clinical indications include:
- Colorectal cancer screening (USPSTF recommends starting at age 45 for average-risk adults)
- Surveillance following prior polyp removal
- Investigation of rectal bleeding or unexplained bowel habit changes
- Inflammatory bowel disease monitoring
- Confirmation after a positive fecal immunochemical test (FIT) or stool DNA test
No competing modality matches this range of capability. Flexible sigmoidoscopy only reaches the distal portion of the colon — roughly the lower 60 cm — missing right-sided lesions entirely. CT colonography covers the full colon but provides no therapeutic capability.
For average-risk individuals with a completely normal examination and no polyps found, USMSTF 2020 guidelines recommend repeating colonoscopy in 10 years — provided the initial exam was high-quality. A high-quality exam is defined in part by the endoscopist's adenoma detection rate (ADR) — a benchmark that varies meaningfully across providers and directly affects how much confidence to place in a negative result.
Preparing for a Video Colonoscopy
Dietary Restrictions and Timeline
Preparation typically begins 1–3 days before the procedure with a low-fiber or clear-liquid diet. Approved clear liquids include water, clear broths, apple juice, sports drinks, and plain tea or coffee.
Avoid liquids dyed red, purple, or orange — these can mimic blood or inflammation on the mucosal surface and complicate interpretation. Most GI facilities also advise avoiding brown-colored beverages, though specific guidance varies by institution, so follow your facility's written prep instructions.
The laxative solution is usually taken the evening before the procedure. For afternoon appointments, split-dose regimens (part the evening before, part the morning of) are increasingly common and tend to improve preparation quality.
Bowel Cleansing Solutions and Medication Adjustments
The dietary phase sets the stage — the laxative regimen does the actual work. Two commonly used preparation categories are:
- Polyethylene glycol (PEG) solutions — high-volume lavage agents, well-studied, safe across most patient groups
- Sodium picosulfate with magnesium citrate (SPMC) — lower-volume alternatives, though kidney function and hydration status factor into whether they're appropriate
Your gastroenterologist selects the prep based on your health history, kidney function, and current medications — clinical factors that override personal preference. Patients taking anticoagulants, NSAIDs, iron supplements, or diabetes medications will typically need to adjust timing or dosing. Do not stop or modify any prescription medication without consulting the prescribing physician first.
Preparation quality is not a convenience issue. Research by Lebwohl et al. published in Gastrointestinal Endoscopy found that suboptimal bowel prep was associated with a 42% overall adenoma miss rate and a 27% advanced adenoma miss rate on repeat colonoscopy. Those numbers represent lesions that could have been caught — and weren't.
How the Video Colonoscopy Procedure Works
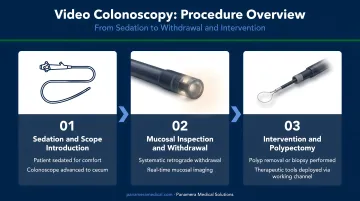
Step 1: Arrival, Sedation, and Positioning
After check-in and a brief pre-procedure assessment, an IV line is placed for sedation. Most procedures in the US use conscious sedation (typically IV midazolam and fentanyl), which keeps patients relaxed and responsive but not fully unconscious. Some facilities use propofol for deeper sedation; unsedated colonoscopy is practiced in some countries, though less common in standard Western clinical settings.
Patients begin in the left lateral decubitus position — lying on the left side with knees gently bent toward the chest. The physician performs a brief digital rectal exam before scope insertion to assess sphincter tone and confirm adequate preparation.
Step 2: Scope Navigation
The endoscopist advances the colonoscope through the sigmoid colon, descending colon, transverse colon, and ascending colon to the cecum, using angulation knobs and gentle torque. Gas (typically CO₂) is insufflated to open the colon walls for visualization. CO₂ is preferred over air: it absorbs faster and reduces post-procedure bloating and discomfort. Some cramping or pressure during the exam is normal and comes from this distension, not from the scope itself.
When the anatomy is difficult to navigate — common in patients with prior surgery or redundant colons — the care team may apply gentle abdominal pressure or ask patients to shift position. These repositioning maneuvers are routine.
Step 3: Withdrawal and Intervention
Most lesions are identified on withdrawal, when the endoscopist slowly retracts the scope while inspecting the mucosal lining. This phase requires patience — withdrawal time serves as a recognized quality indicator for procedural thoroughness.
During withdrawal, several interventions can occur in the same session:
- Polypectomy — snare or forceps removal of polyps
- Biopsy — tissue sampling of suspicious areas
- Clip placement — for bleeding control
- Chromoendoscopy — contrast dye application to enhance mucosal visualization
Modern high-definition video colonoscopes, and increasingly AI-assisted detection systems, have improved adenoma detection rates — particularly for lesions in the 1–5 mm range. For facilities evaluating equipment upgrades, this detection capability is a meaningful clinical differentiator worth factoring into procurement decisions.
Understanding Your Video Colonoscopy Results
Results arrive in two phases.
Immediately after the procedure, the physician provides a verbal summary: what was seen, whether polyps were removed, and any gross findings such as diverticula or signs of inflammation.
Lab results from biopsies or removed tissue take longer. Turnaround varies by facility — Mayo Clinic references a few days to 1–2 weeks; the NHS cites up to 2–3 weeks. Ask your care team for the expected timeline before you leave.
What Findings Mean
| Finding | Meaning | Typical Follow-Up |
|---|---|---|
| Normal (no polyps) | No abnormalities detected | Repeat in 10 years (average risk) |
| Hyperplastic polyps (≤20, <10mm, rectosigmoid) | Generally benign | Treated as low-risk; ~10-year interval |
| 1–2 tubular adenomas <10mm | Precancerous; removed | 7–10 years |
| 3–4 tubular adenomas <10mm | Precancerous; removed | 3–5 years |
| 5–10 adenomas or advanced features | Higher-risk findings | 3 years |
| Colorectal carcinoma or IBD signs | Requires further workup | Individualized clinical plan |
These results assume a complete exam. When the scope doesn't reach the cecum — due to looping, inadequate preparation, or patient anatomy — the physician may recommend a repeat procedure with an adjusted technique, CT colonography, or referral to a specialist with advanced equipment.
Post-Procedure Symptoms to Watch
- Normal: Mild bloating and gas, typically resolving within hours
- See a doctor promptly: Rectal bleeding persisting beyond a day, fever, or severe abdominal pain — these may indicate rare but serious post-polypectomy complications
Key Factors That Affect Video Colonoscopy Quality
Four variables determine how accurate and safe a colonoscopy will be:
- Bowel preparation quality — the most patient-controllable factor (see prep section above)
- Endoscopist experience and ADR — the ASGE/ACG Quality Task Force (2024) sets the minimum acceptable adenoma detection rate at 35% for patients aged 45+ across screening, surveillance, and diagnostic colonoscopies
- Equipment generation and image quality — a peer-reviewed study found that latest-generation wide-angle HD colonoscopes increased ADR by 22% compared with mixed older-technology units
- Adjunct imaging technologies — narrow-band imaging (NBI) and chromoendoscopy enhance mucosal contrast, with the strongest evidence supporting their use in high-risk or surveillance populations rather than routine average-risk screening
Equipment Quality Is Not a Fixed Variable
Facilities operating aging colonoscope fleets face a real diagnostic trade-off. Older or poorly maintained endoscopes can degrade image resolution, reduce detection rates, and increase procedural risk. The ADR data above reflects a measurable performance gap tied directly to equipment generation — facilities don't have to absorb those losses passively.
For facilities weighing the cost of a full fleet replacement, the pre-owned and refurbished market offers a practical middle path. Companies like Panamera Medical Solutions specialize in colonoscope trade-in and buy-back programs, allowing facilities to apply trade-in value toward newer-generation units or recover capital from equipment no longer in active use.
When Colonoscopy May Not Be the Right Choice
- Active severe colitis or suspected perforation — contraindications for routine colonoscopy
- Adults over 75 — USPSTF recommends individualized decision-making, not a blanket cutoff; the risk-benefit balance shifts as comorbidities accumulate and prior screening history factors in
- When less invasive alternatives are preferred — FIT, stool DNA testing, or CT colonography may be more appropriate for certain patient profiles
Frequently Asked Questions
What is a video colonoscope?
A video colonoscope is a flexible endoscopic instrument with a digital CCD or CMOS sensor at its distal tip that transmits live, high-definition images to an external monitor. This distinguishes it from older fiber-optic models, which relay images through glass fiber bundles at lower resolution and without real-time digital display.
How long does colonoscopy prep take — will I be on the toilet all night?
The purging effect varies by product and individual, but most patients complete the active preparation phase within a few hours of taking the laxative solution — not throughout the entire night. Split-dose regimens, where part of the prep is taken the morning of an afternoon procedure, are increasingly common and can make the experience more manageable.
What position are you in during a colonoscopy?
Patients begin lying on their left side with knees gently bent — called the left lateral decubitus position — which makes initial scope insertion easier. The care team may ask you to shift position during the procedure to help the endoscopist navigate loops in the colon.
Why do doctors stop recommending colonoscopies after age 75?
Age 75 isn't a hard cutoff. USPSTF recommends individualized decision-making for adults 76–85, balancing procedural risks — sedation complications, perforation — against whether detecting a slow-growing cancer at this stage would meaningfully affect life expectancy. Prior screening history and overall health both factor in.
How is video colonoscopy different from virtual colonoscopy?
Video colonoscopy uses a physical scope for direct visualization and allows immediate intervention — polyp removal, biopsy, clip placement — all in one session. Virtual colonoscopy (CT colonography) uses X-ray imaging to create a 3D colon map without scope insertion, but any polyp detected still requires a standard colonoscopy for removal.
How long does the procedure take from start to finish?
The scope insertion and examination phase typically takes 30–60 minutes depending on findings and anatomy. Including check-in, sedation, and recovery, plan to spend 2–3 hours at the facility. You'll need someone to drive you home — sedation disqualifies you from driving for the rest of the day.