Doctors recommend bronchoscopy for a range of reasons: a chronic cough lasting more than 8 weeks, unexplained shortness of breath, coughing up blood, or an abnormal finding on a chest X-ray or CT scan. According to a 2021 peer-reviewed study, over 500,000 bronchoscopies are performed each year in the United States — making it one of the most common pulmonary procedures.
This article answers four key questions: what bronchoscopy is used for, the different types available, exactly what happens during the procedure, and what to expect from risks, results, and recovery.
Key Takeaways
- Bronchoscopy provides direct airway visualization and tissue sampling that CT scans cannot offer
- Flexible bronchoscopy is the most common type; rigid and EBUS are used for specific clinical needs
- Fasting is required beforehand, and certain blood-thinning medications must be paused beforehand
- Serious complications occur in fewer than 1% of flexible bronchoscopy cases
- Most patients go home the same day and return to normal activities the following day
What Is Bronchoscopy and What Is It Used For?
A bronchoscopy is an endoscopic procedure performed by a pulmonologist or thoracic specialist. The bronchoscope (a thin, lighted tube with a camera) is guided through the nose or mouth, past the vocal cords, and into the bronchial airways to directly visualize the lungs.
Diagnostic Indications
A doctor may order bronchoscopy to investigate:
- Chronic cough lasting more than 8 weeks in adults (per ERS guidelines)
- Unexplained shortness of breath
- Coughing up blood (hemoptysis)
- Abnormal findings on a chest X-ray or CT scan
- Suspected lung infection, particularly in immunocompromised patients
Therapeutic Indications
Beyond diagnosis, bronchoscopy can also treat conditions directly:
- Removing foreign bodies or mucus plugs obstructing the airway
- Placing stents to keep narrowed airways open
- Cauterizing bleeding tumors to control hemoptysis
- Draining lung abscesses
How Bronchoscopy Compares to a CT Scan
A CT scan can confirm an abnormality exists, but it cannot identify what the abnormality is. Bronchoscopy fills that gap by allowing the physician to collect tissue and fluid samples for a definitive pathology result. Research published in Thorax found bronchoscopy was diagnostic in 73% of suspected lung cancer cases when CT was reviewed beforehand, compared to 54% when bronchoscopists had no prior CT review — a significant difference that highlights why the two tools work best together.
Conditions bronchoscopy can detect include:
- Lung cancer and pulmonary fibrosis
- Tuberculosis and other lung infections
- Sarcoidosis and interstitial lung disease
- Airway strictures and post-transplant rejection
Types of Bronchoscopy: Flexible, Rigid, EBUS, and Beyond
Not all bronchoscopies are the same. The procedure chosen depends on where the problem is, what the doctor needs to do, and how complex the intervention will be.
Flexible Bronchoscopy
The most common type. A thin, bendable tube is passed through the nose or mouth — no general anesthesia required. It can reach smaller, peripheral airways that rigid scopes cannot access, making it the preferred option for:
- Airway inspection and visualization
- Bronchoalveolar lavage (BAL) — fluid sampling for infection analysis
- Tissue biopsies using forceps or brushes
- Moderate therapeutic work
Rigid Bronchoscopy
A firm, straight metal tube inserted under general anesthesia. Rigid bronchoscopy is reserved for cases requiring more forceful intervention:
- Removing large foreign bodies
- Treating massive hemoptysis
- Deploying airway stents
- Debulking tumors blocking central airways
It offers a wider working channel than flexible scopes, which is essential for these higher-intensity procedures.
Endobronchial Ultrasound (EBUS)
EBUS combines a bronchoscope with a built-in ultrasound probe to sample lymph nodes adjacent to the airways — critical for cancer staging.
- Linear EBUS: Provides real-time ultrasound guidance for needle biopsy of mediastinal lymph nodes. A meta-analysis of 1,299 patients found pooled sensitivity of 0.93 for detecting metastatic lymph nodes in lung cancer.
- Radial EBUS: Uses 360-degree ultrasound visualization to localize peripheral lung lesions before sampling.
Navigational and Robotic Bronchoscopy
Standard flexible bronchoscopy struggles to reach small peripheral nodules. Newer platforms address this directly:
- Navigational bronchoscopy uses electromagnetic guidance derived from CT imaging. A 2023 meta-analysis reported a pooled diagnostic yield of 71.1% for peripheral pulmonary nodules.
- Robotic bronchoscopy adds robotic-assisted precision, with a pooled diagnostic yield of 80.4% in a 2024 meta-analysis — compared to just 25.6% with standard non-guided flexible bronchoscopy.
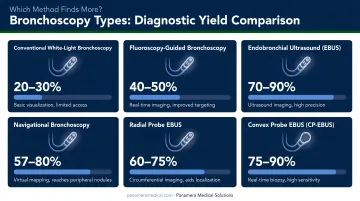
These cross-study benchmarks aren't direct head-to-head comparisons, but the gap between 25.6% and 80.4% diagnostic yield signals a real clinical difference — one that's pushing many facilities to reassess their bronchoscope inventory.
That upgrade decision carries a capital question. Moving from older standard scopes to video or robotic platforms is expensive, and many facilities need a path that offsets the cost. Panamera Medical Solutions works with healthcare facilities on trade-in and buy-back programs for bronchoscopes from brands including Olympus, Pentax, Fujifilm, Karl Storz, and Stryker. Older equipment is recouped at value and applied toward the next generation of platforms.
How to Prepare for a Bronchoscopy
Good preparation reduces your risk of complications and helps the care team work efficiently. Expect to address four areas: fasting, medications, logistics, and imaging.
Fasting Requirements
Per the 2019 Guidelines for Diagnostic Flexible Bronchoscopy in Adults, patients should fast for at least 2 hours for clear liquids and 4 hours after a light meal before the procedure. Fatty foods may require 8 or more hours. Always follow your specific facility's instructions, as policies vary.
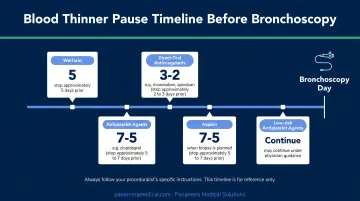
Medications to Pause
Blood thinners require advance planning:
- Warfarin: Stop 5 days before the procedure
- Clopidogrel: Stop 5–7 days before transbronchial biopsy
- Direct oral anticoagulants (DOACs): Typically 1–2 days interruption; up to 3–5 days for dabigatran if kidney function is reduced
- Low-dose aspirin alone: Can generally be continued — confirm with your doctor
Logistical Checklist
- Arrange a driver — sedation prevents you from driving yourself home
- Bring a full list of current medications and known allergies
- Remove dentures and hearing aids on the day of the procedure
- Plan to rest for the remainder of the day afterward
Pre-Procedure CT Scan
In most non-emergency cases, a CT scan is performed before bronchoscopy. It helps the pulmonologist locate abnormalities, choose the right bronchoscope type, and map the approach before entering the airway.
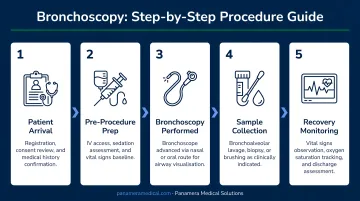
What Happens During a Bronchoscopy: Step by Step
Here is what patients and care teams can expect, from arrival through recovery.
Step 1 — Arrival and monitoring setup The patient is positioned on a procedure table. IV access is established, and monitoring equipment tracking oxygen saturation and blood pressure is connected. ECG monitoring is added for patients with cardiac risk factors.
Step 2 — Sedation and anesthesia A sedative is administered through the IV, and a numbing spray is applied to the nose or throat. Anesthesia type depends on the procedure:
- Flexible bronchoscopy: Moderate IV sedation — patients are relaxed and drowsy but able to respond
- Rigid bronchoscopy: Full general anesthesia required
Most patients remember little to nothing of the procedure.
Step 3 — Scope insertion and airway inspection The bronchoscope is guided through the nose or mouth, past the vocal cords, and down into the bronchial airways. The camera transmits live images directly to a monitor, giving the pulmonologist a clear view of airway walls for signs of narrowing, bleeding, or blockages.
Step 4 — Sampling and intervention Depending on the purpose, the provider may:
- Perform BAL — flushing sterile saline into a lung segment and collecting fluid for culture or cell analysis
- Take tissue biopsies using forceps or a needle
- Use EBUS guidance for lymph node sampling
- Place a stent or perform another therapeutic intervention
Step 5 — Recovery monitoring Once the scope is removed, the patient moves to a recovery area for 45–60 minutes while sedation clears. Eating and drinking must wait until throat numbness fully resolves — typically 1–2 hours post-procedure — to prevent aspiration. For symptomatic patients, a chest X-ray is ordered to rule out pneumothorax.
Bronchoscopy Risks and Complications
Bronchoscopy has a strong safety profile, but knowing the difference between normal side effects and genuine complications helps patients respond appropriately.
Common, Self-Resolving Side Effects
These are normal and typically resolve within a few days:
- Sore throat or hoarse voice for 24–48 hours
- Mild cough
- Blood-tinged mucus for 2–3 days after biopsy
Uncommon Procedural Risks
According to the 2019 flexible bronchoscopy guidelines, serious adverse events occur in fewer than 1% of cases. Specific risks include:
- Bleeding: Overall incidence 0.19%; up to 7.5% in patients with clotting abnormalities
- Pneumothorax: Air entering the space around the lung; occurs in 1–6% of cases involving transbronchial lung biopsy, rarely requiring surgery
- Post-procedure fever: Reported in 0.9–2.5% of procedures; not always a sign of infection
- Mortality: Large retrospective series report rates of 0.02–0.1%
When to Seek Immediate Care
Contact your care team or go to an emergency department if you experience:
- Chest pain or sudden difficulty breathing
- Persistent or worsening shortness of breath
- Coughing up more than small amounts of blood, or blood that doesn't stop
- Fever with chills that develops after the procedure
These warning signs matter more for some patients than others. Those with significant cardiovascular disease, unstable arrhythmias, or a recent myocardial infarction face higher procedural risk and need thorough evaluation before the procedure.
Bronchoscopy Results and Recovery
Understanding Your Results Timeline
Results don't all come back at the same time:
- Direct visual findings: Often shared immediately after the procedure or within 1–3 days
- Biopsy pathology: Mayo Clinic notes that results are typically discussed 1–3 days after the procedure
- Molecular or genetic profiling of cancer tissue: Up to 10 working days, per CAP/IASLC/AMP benchmarks
Waiting on pathology is a standard part of the process. A delayed result reflects lab workflow, not a complication.
What Abnormal Results Can Mean
Once results are in, abnormal findings shape what comes next. Bronchoscopy results may indicate:
- Lung cancer — tissue collected for molecular profiling to determine targeted treatment options
- Infection — bacterial, fungal, viral, or tuberculosis identified through BAL culture
- Interstitial lung disease or sarcoidosis — confirmed through lavage cellular analysis
- Airway stricture — narrowing that may require stenting or further intervention
- Post-transplant rejection — detected through transbronchial biopsy in lung transplant recipients
Recovery Expectations
Most bronchoscopies are outpatient procedures. Patients can generally expect:
- Fatigue for the remainder of the day is common
- Avoid driving until the following day at minimum
- Most patients return to normal activities the day after the procedure
- Therapeutic bronchoscopy patients may need additional recovery time depending on what was done
Frequently Asked Questions
Is it painful having a bronchoscopy?
Bronchoscopy is not painful — the lungs have no pain receptors, and sedation is administered before the scope is inserted. Patients may feel brief pressure or mild discomfort as the scope passes the vocal cords, but the numbing medication resolves this quickly.
Is a bronchoscopy a serious procedure?
The risk level depends on the type. Airway inspection and BAL carry lower procedural risk; transbronchial biopsy and therapeutic bronchoscopy are higher-risk categories. It is less invasive than open surgery or thoracoscopy, but more involved than a standard outpatient endoscopy.
How long does a bronchoscopy usually take?
According to MD Anderson, diagnostic bronchoscopy for a lung nodule typically takes 45 minutes to 1 hour; BAL alone can take 10–20 minutes; therapeutic bronchoscopy may take 1–2 hours. Factor in preparation and recovery when planning your total time at the facility.
Do they put you to sleep for a bronchoscopy?
Most patients receive moderate IV sedation — sleepy and relaxed, but not fully unconscious. General anesthesia is used for rigid bronchoscopy and more complex procedures. Either way, most patients have little to no memory of the procedure.
How long does it take to recover from a bronchoscopy?
Patients spend 45–60 minutes in the recovery area before discharge. Fatigue is common for the rest of that day, but most people return to normal activities the following morning. You'll need someone to drive you home and stay with you for the remainder of the day.
What can a bronchoscopy detect?
Bronchoscopy can diagnose lung cancer, tuberculosis and other lung infections (bacterial, fungal, viral), interstitial lung disease, sarcoidosis, airway blockages or strictures, and acute rejection in lung transplant recipients.