Introduction
In 2015, a contaminated reusable duodenoscope at UCLA Medical Center triggered a carbapenem-resistant Enterobacteriaceae (CRE) outbreak that infected more than 170 patients. The CDC later confirmed the device's complex elevator mechanism had harbored bacteria that survived standard reprocessing — a finding that forced the entire GI community to reconsider its assumptions about endoscope safety.
That outbreak wasn't an isolated incident. The FDA has documented 4–6% high-concern organism contamination rates in older reprocessed duodenoscope models, and in April 2022, the agency issued a formal safety communication recommending that facilities transition to duodenoscopes with disposable components or fully disposable designs.
That regulatory pressure accelerated a shift already underway. Single-use endoscopy has moved quickly from niche to mainstream — what began with cholangioscopy now spans full single-use duodenoscopes (FDA-cleared in December 2019), bronchoscopes, cystoscopes, ureteroscopes, and gastroscopes.
This guide covers the decisions procurement teams and clinical leaders face today: clinical performance data, real cost comparisons, operational implications, environmental tradeoffs, and a framework for evaluating what fits your facility's specific volume and risk profile.
Key Takeaways
- FDA recommends transitioning away from fixed-endcap reusable duodenoscopes toward disposable or innovative designs
- Reprocessing costs run $114–$281 per scope cycle — costs that disappear entirely with single-use
- Single-use duodenoscope costs range from $1,995 to $4,400 per unit, making procedure volume the critical financial variable
- Waste increases by ~40% with full single-use adoption, though reprocessing generates its own substantial environmental burden
- Decommissioned reusable scopes retain resale value, and trade-in or buy-back programs help facilities offset transition costs
What Are Single-Use Endoscopy Systems?
Single-use (disposable) endoscopes are sterile, pre-packaged devices designed for one patient procedure and then discarded. They connect to a reusable controller or processor that handles image capture and output — substantially reducing the capital investment compared to traditional setups, though not eliminating it entirely.
How They Work
Unlike conventional endoscopy suites where the scope itself represents the major capital asset, single-use systems shift the cost structure: the reusable processor stays in place, and the insertable scope is replaced per procedure. This architecture simplifies infection control because the component most likely to harbor residual contamination is discarded after each use.
The Technology Timeline
The category has evolved rapidly:
- 2015: SpyGlass DS Direct Visualization System launched for cholangioscopy
- December 2019: EXALT Model D receives first FDA 510(k) clearance for a single-use duodenoscope (K193202)
- 2021–present: Single-use gastroscopes, bronchoscopes, cystoscopes, and ureteroscopes reach commercial availability
FDA-cleared single-use categories now span multiple specialties:
- Duodenoscopes: EXALT Model D
- Gastroscopes: Ambu aScope Gastro
- Bronchoscopes: Ambu aScope 4 Broncho
- Ureteroscopes: LithoVue Elite
A peer-reviewed randomized study confirmed the Ambu single-use flexible cystoscope was noninferior to reusable alternatives across procedure completion, image quality, and maneuverability.
Key Advantages of Single-Use Endoscopy Systems
Infection Control
This is where the clinical case is strongest. Reprocessing complex duodenoscopes involves an elevator mechanism with tight tolerances that cleaning agents and brushes cannot reliably reach. The FDA's own surveillance data found 4–6% of reprocessed duodenoscopes harbored high-concern organisms even after following manufacturer reprocessing instructions.
Eliminating reprocessing eliminates that exposure pathway entirely.
Reprocessing Burden Eliminated
The labor involved in reprocessing a single flexible endoscope is substantial:
- 100+ distinct procedural steps per scope
- 76 minutes average hands-on staff time per cycle
- $114–$281 reprocessing cost per scope (per Boston Scientific cost analysis)
- An additional $52–$68 per scope in new compliance activities, per a 2024 peer-reviewed study
- Ongoing staff training and competency verification requirements for each scope model

Single-use systems eliminate each of these line items from the equation.
Operational Flexibility
Single-use scopes are always ready. No cleaning cycle delays, no scopes out for repair, no scheduling gaps from unplanned downtime. For urgent bedside bronchoscopies, after-hours emergency ERCP, or hybrid OR settings where sterile conditions are required, that on-demand readiness directly protects procedure scheduling.
The time savings extend beyond availability. A 2024 workflow study found single-use cystoscopes reduced pre- and post-procedure hands-on labor by 48% compared to reusable alternatives — nearly 2.5 minutes per case, which compounds significantly across high-volume days.
Expanded Care Settings
The self-contained, no-reprocessing-infrastructure model makes single-use endoscopy practical in:
- Ambulatory surgery centers with limited processing space
- Remote or rural facilities
- Bedside ICU procedures
- Clinics where full endoscopy suite infrastructure isn't available
These advantages are real and clinically meaningful — but they come with tradeoffs in cost, image quality, and environmental impact that procurement teams need to weigh carefully.
Drawbacks and Limitations to Consider
Per-Unit Cost
The device cost for single-use endoscopes is higher than the amortized per-procedure cost of reusable scopes at volume centers. A 2022 peer-reviewed review reported retail prices of $1,995 for the Ambu aScope Duodeno and up to $4,400 for the EXALT Model D, compared to the outline's referenced range of $200–$550 amortized per procedure for reusable duodenoscopes at high-volume centers.
That gap narrows considerably once reprocessing labor, maintenance contracts, and compliance costs are factored into the reusable side of the ledger.
Procedural Complexity Limitations
Early-generation single-use duodenoscopes had documented limitations in reach and pushability compared to high-end reusable systems. A first-generation single-use duodenoscope cohort study reported 90.4% ERCP completion rates, rising to 94.2% over time — acceptable for most cases but worth evaluating against your facility's case complexity mix. Procedures involving highly altered anatomy (post-Whipple, Roux-en-Y) continue to be studied.
Storage and Supply Chain
High daily volume means stocking substantial quantities of boxed scopes. Facilities with limited storage space — particularly smaller ASCs — should model their daily scope volume against available storage capacity before committing to a full transition.
Medical Waste
A Gut 2022 study estimated that each endoscopic procedure already generates approximately 4.6 lbs (2.1 kg) of disposable waste. A full shift to single-use endoscopes would increase net waste mass by roughly 40%. For sustainability-conscious health systems, this is a real constraint to weigh.
Adoption and Learning Curve
Even well-designed single-use scopes feel different from familiar reusable systems. The transition introduces several friction points:
- Ergonomic differences in handle design and deflection controls
- Tactile feedback changes that affect navigation feel during procedures
- Institutional inertia from staff accustomed to familiar reusable workflows
Structured physician training programs and phased rollouts reduce ramp-up time — most facilities report stabilized performance metrics within 30–60 cases per endoscopist.
Cost Analysis: Single-Use vs. Reusable Endoscopes
The True Cost of "Cheaper" Reusable Scopes
The purchase price of a reusable scope is only one line item. A complete cost-per-procedure calculation for reusable systems must include:
- Reprocessing labor: $114–$281 per cycle
- New compliance activities: an additional $52–$68 per scope per a 2024 study
- Repair and maintenance contracts
- Capital depreciation over the scope's service life
- Staff training and competency verification costs
- Costs associated with scope-related infection events (investigation, litigation, reputation)
When these factors are included, the economic advantage of reusable scopes at moderate volumes shrinks substantially.
Volume is the decisive variable. High-volume centers performing 150+ ERCPs annually spread reusable scope costs more effectively, keeping per-procedure costs low. For centers performing 50 or fewer ERCPs annually, single-use can be cost-competitive or cheaper once full-cycle costs are accounted for.
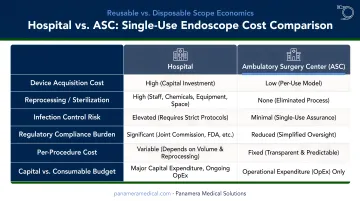
Hospital vs. Ambulatory Surgery Center Economics
| Factor | Hospital/Health System | Ambulatory Surgery Center |
|---|---|---|
| Volume | Higher — better cost amortization for reusables | Lower — less purchasing leverage |
| Storage | More capacity | Often limited |
| Reimbursement | CMS Transitional Pass-Through (HCPCS C1748) available | May apply in ASC context too |
| Reprocessing infrastructure | Full sterile processing departments | Often limited or outsourced |
| Break-even likelihood | Favors reusable at very high volume | Single-use often competitive when fully costed |
Large health systems can also negotiate volume pricing for single-use scopes. The CMS Transitional Pass-Through reimbursement (HCPCS code C1748) has applied to single-use upper GI endoscopes since July 1, 2020 — a detail worth confirming with your billing team when building the financial case.
Recovering Value from Decommissioned Reusable Scopes
For facilities making the transition, existing reusable endoscopes aren't a write-off — they retain real market value. Panamera Medical Solutions' trade-in and buy-back programs allow healthcare organizations to sell or trade decommissioned Olympus, Pentax, Fujifilm, Karl Storz, and Stryker scopes through an international trading network.
Facilities have two options:
- Receive credit toward newer-generation equipment
- Take a cash payment for unwanted scopes and video systems
For a procurement officer building the financial case for transitioning to single-use, that recovered value directly reduces the net transition cost.
Environmental Impact and Sustainability Considerations
The waste numbers are sobering. U.S. endoscopy generates an estimated 38,000 metric tons of waste annually across 18 million procedures, and a complete shift to single-use endoscopes would increase net waste mass by ~40%, with waste from reprocessing and scope disposal potentially quadrupling if ancillary supplies are excluded.
That said, the full lifecycle picture is more nuanced than the plastic waste headline suggests.
Reprocessing Has Its Own Footprint
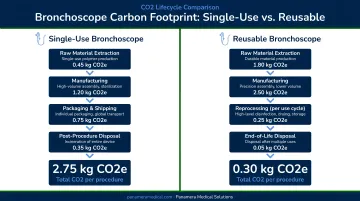
Reprocessing consumes disinfectant chemicals, water, energy, personal protective equipment, and packaging materials — none of which appear in simple waste-per-procedure comparisons. A CHEST 2024 study reported single-use bronchoscopes at 3.9 kg CO₂e per procedure versus reusable bronchoscopes at 2.9 kg CO₂e — a real difference, but smaller than raw waste figures imply when reprocessing inputs are factored in.
What's Changing
- Ambu's Recircle program collects and recycles used single-use endoscopes
- Material innovations are underway, including bioplastic components in newer devices
- Lifecycle assessment standards are still evolving, so facilities should revisit sustainability comparisons as updated data emerges
The environmental calculus depends heavily on procedure volume, reprocessing infrastructure, and what gets counted. Neither system holds a clean advantage across every scenario.
How to Decide: Is Single-Use Right for Your Facility?
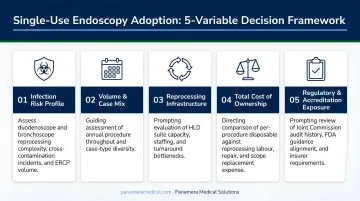
Five Variables to Assess
Before committing to a direction, evaluate these factors:
- Procedure volume by scope type — How many ERCPs, bronchoscopies, or cystoscopies per year? Volume thresholds shift the cost math significantly
- Current reprocessing cost and staffing capacity — Are you fully accounting for labor, compliance, and repair costs?
- Infection history and regulatory pressure — Prior contamination events or accreditation concerns may accelerate the transition to single-use
- Available storage space — High-volume single-use adoption requires dedicated, organized inventory space
- Patient population risk profile — Immunocompromised patients, post-surgical anatomy, or outbreak-sensitive environments all weight toward single-use
A Staged Adoption Approach
Most facilities aren't facing a binary all-or-nothing choice. A practical hybrid approach might look like this:
- Transition first: Bronchoscopes and cystoscopes — both operationally disruptive to reprocess, with strong single-use clinical evidence and meaningful workflow efficiency gains
- Transition next: Duodenoscopes — FDA guidance is clear, and the infection risk case is compelling
- Evaluate later: High-volume colonoscopy and gastroscopy lines, where reusable scope economics remain favorable at volume
Facilities can sell off select inventory — bronchoscopes or cystoscopes, for example — while retaining reusable colonoscopes. There's no requirement to decommission everything at once. Panamera Medical Solutions supports partial fleet transitions, connecting decommissioned equipment with buyers across North America, Europe, and South America.
Frequently Asked Questions
Are single-use endoscopes as effective as reusable ones for complex procedures?
Peer-reviewed trials show noninferior performance for single-use flexible cystoscopes, and clinical series report 90–94% ERCP completion rates for single-use duodenoscopes across mixed-complexity cases. Some endoscopists still prefer high-end reusable systems for the most technically demanding or anatomically complex procedures.
What does the FDA recommend regarding single-use vs. reusable duodenoscopes?
The FDA's April 5, 2022 safety communication formally recommends that healthcare facilities transition to duodenoscopes with disposable components or fully disposable designs. This follows earlier 2019 guidance after FDA surveillance found 4–6% contamination rates with high-concern organisms in reprocessed fixed-endcap duodenoscope models.
How much do single-use endoscopes cost compared to reusable ones?
Single-use duodenoscopes retail between $1,995 and $4,400 per unit. A fair comparison must include reprocessing labor ($114–$281 per cycle), compliance costs, and repair contracts — at low-to-moderate procedure volumes, single-use is often cost-competitive once the full cost stack is calculated.
Which types of endoscopes are currently available as single-use?
FDA-cleared single-use options include duodenoscopes, gastroscopes, bronchoscopes, and ureteroscopes. Clinical evidence supports single-use flexible cystoscopes as well. Duodenoscopes and bronchoscopes represent the most widely adopted categories, driven by infection control urgency and workflow efficiency gains respectively.
Are single-use endoscopes worse for the environment than reusable ones?
Single-use endoscopes generate more solid waste per procedure — a full transition could increase net waste by ~40%. Reprocessing, however, carries its own footprint in chemicals, water, energy, and PPE, and lifecycle analyses show the actual gap is smaller than raw plastic figures suggest, especially with manufacturer recycling programs now available.
What should a facility do with existing reusable endoscopes when transitioning to single-use?
Reusable scopes from major manufacturers retain real market value and shouldn't simply be decommissioned. Specialized endoscopy equipment trading companies like Panamera Medical Solutions offer buy-back and trade-in programs, connecting decommissioned inventory with buyers across North America, Europe, and South America — giving facilities working capital or equipment credit instead of absorbing the loss.