Introduction
Linear EUS is one of the few diagnostic tools that delivers both high-resolution imaging and real-time tissue acquisition in a single procedure. While radial EUS maps anatomy in a 360-degree sweep, the linear array configuration is what makes guided biopsy, drainage, and intervention possible — making it the instrument of choice for pancreatic, biliary, and mediastinal workups.
For clinicians, the clinical indications can blur — particularly when deciding between linear and radial approaches, or when determining whether EUS-FNA or EUS-FNB is appropriate. For procurement teams and biomedical engineers, the equipment variables add another layer: probe compatibility, processor generation, and scope condition all affect procedural reliability.
This article covers the underlying technology, primary clinical indications, procedural workflow, safety profile, and practical considerations for facilities sourcing or upgrading linear EUS equipment.
Key Takeaways
- Linear EUS scans parallel to the scope axis, keeping needles in the imaging plane for real-time guidance
- Linear EUS supports both diagnosis and intervention, including FNA, FNB, and cyst drainage — capabilities radial EUS cannot offer
- Core indications include pancreatic lesion evaluation, GI cancer staging, biliary assessment, and submucosal tumor characterization
- Most patients receive moderate sedation; recovery to normal activity typically takes under 24 hours
- When sourcing linear EUS equipment, evaluate image quality, processor compatibility, working channel diameter, and total cost of ownership
What Is Linear Endoscopic Ultrasound?
Linear EUS is a minimally invasive procedure that combines a flexible endoscope with a high-frequency ultrasound transducer mounted at the scope tip. The key distinction from other EUS variants is its scanning geometry: the transducer images in a plane parallel to the long axis of the instrument, producing a forward-oblique sector view rather than a 360° cross-sectional slice.
How the Imaging Plane Enables Needle Guidance
That parallel orientation is the defining feature. When a needle is advanced through the scope's accessory channel into adjacent tissue, it travels within the same plane the transducer is imaging — meaning the endoscopist can watch it advance in real time under continuous ultrasound guidance. This is what makes linear EUS the platform for interventional procedures like fine needle aspiration (FNA), fine needle biopsy (FNB), and therapeutic drainage.
That guidance capability depends on operating frequency. Linear echoendoscopes typically operate at 5–12 MHz, with higher frequencies providing greater resolution at the cost of penetration depth.
Because the transducer sits directly against the GI wall (often with a water-filled balloon for acoustic coupling), the images achieve close-proximity resolution that external ultrasound, CT, or MRI cannot consistently match for structures like the pancreatic parenchyma.
Anatomical Access
From different positions along the GI tract, linear EUS can reach a wide range of structures:
- From the esophagus and stomach: pancreas (head, body, tail), celiac axis, left lobe of the liver, mediastinal lymph nodes, adrenal glands, bile ducts, gallbladder
- From the duodenum: pancreatic head and ampullary region
- From the rectum (lower EUS): perirectal structures, pelvic lymph nodes
Trained gastroenterologists or endosonographers perform these procedures. The dual diagnostic-therapeutic capability means linear EUS frequently replaces what would otherwise be two separate sessions — an imaging study followed by a guided biopsy.
Linear vs. Radial EUS: Key Differences
Linear and radial EUS differ fundamentally in how they orient the image plane — and that difference determines what each scope can do clinically.
Radial EUS uses a transducer that rotates perpendicular to the scope axis, generating a 360° cross-sectional image (similar to a CT "slice") with the scope as the central reference point. This orientation is intuitive for physicians trained on CT imaging and provides an excellent anatomical overview, particularly for assessing GI wall layer involvement in cancer staging.
The practical distinction comes down to what each scope can do clinically:
| Feature | Linear EUS | Radial EUS |
|---|---|---|
| Scanning plane | Parallel to scope axis | Perpendicular to scope axis |
| Image orientation | Longitudinal sector view | 360° cross-sectional view |
| Needle guidance | Real-time, in-plane | Not standard for needle guidance |
| Working channel | Large (e.g., 3.7–4.0 mm) | Limited (e.g., 2.2 mm on some models) |
| Primary use | Diagnosis + therapeutic intervention | Anatomical staging and overview |
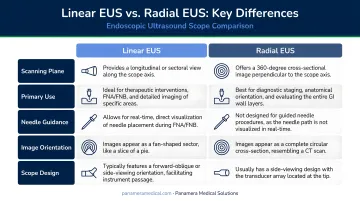
A note on working channels: not all radial scopes lack a channel entirely — some have limited ones — but radial EUS is not the standard platform for real-time needle-guided procedures. Linear EUS fills that role.
Training Considerations
Historically, many endoscopists trained on radial EUS first — but that's changing. Current guidance and program design now reflect three key shifts:
- ESGE designates linear EUS training as mandatory, with radial as a complement where available
- Prior radial training does not meaningfully improve subsequent linear EUS performance
- Most programs now adopt linear-first curricula based on this evidence
Clinical Applications of Linear EUS
Pancreatic Evaluation
Linear EUS is the imaging method of choice for the pancreas at close range. A 2019 review reported EUS sensitivity of 94% overall for pancreatic tumors — and for lesions ≤20 mm, EUS achieved 94.4% sensitivity compared to 50.0% for contrast CT. That gap matters clinically: small pancreatic lesions are where early detection changes outcomes.
Beyond masses, linear EUS evaluates:
- Chronic pancreatitis — EUS detects parenchymal and ductal changes that CT and ERCP can miss, with EUS elastography showing diagnostic accuracy of approximately 91%
- Pancreatic cysts and IPMNs — EUS-guided cyst fluid analysis provides CEA and glucose measurements that help distinguish mucinous from non-mucinous lesions
- Pancreatic adenocarcinoma — including local extent and vascular involvement
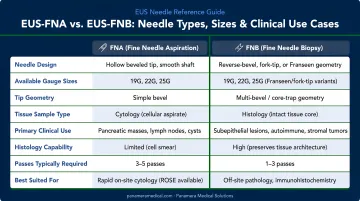
EUS-Guided Tissue Acquisition (FNA and FNB)
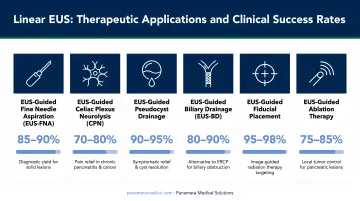
FNA and FNB are among the most common interventional applications. A needle passed through the accessory channel is guided in real time into a lesion, lymph node, or mass for sampling. Classic EUS-FNA data for pancreatic masses reported 89.5% sensitivity, 98.4% specificity, and 91.5% diagnostic accuracy.
FNB needles — including Franseen, fork-tip, and reverse-bevel designs — retrieve intact core tissue rather than cytological material alone. FNB is preferred when histologic architecture matters, particularly for:
- Autoimmune pancreatitis diagnosis
- Lymphoma evaluation
- Subepithelial lesion characterization
These cases benefit from preserved tissue architecture that FNA cytology cannot reliably provide.
Common needle sizes span 19G, 22G, and 25G, with selection based on target location, lesion characteristics, and required sample type.
Cancer Staging
Linear EUS contributes to T-staging (local tumor extent) and N-staging (regional lymph node involvement) for esophageal, gastric, pancreatic, and rectal cancers. For esophageal cancer, EUS achieves approximately 85% T-staging accuracy and >70% N-staging accuracy.
Distinguishing malignant from benign nodes relies on echo features:
| Feature | Malignant Nodes | Benign Nodes |
|---|---|---|
| Echogenicity | Hypoechoic | Mixed |
| Shape | Round | Irregular |
| Margins | Sharp | Indistinct |
Echo features alone are not definitive. When nodal status would change treatment — such as determining surgical eligibility — EUS-FNA adds cytologic confirmation to the assessment.
Biliary and Gallbladder Assessment
ASGE's pooled data reports EUS sensitivity of 0.97 and specificity of 0.90 for choledocholithiasis — outperforming transabdominal ultrasound and CT for bile duct stones, including microlithiasis and biliary sludge that other modalities miss.
When ERCP fails or is not feasible for biliary obstruction, EUS-guided biliary drainage (EUS-BD) serves as a reliable alternative. ESGE recommends EUS-BD over percutaneous transhepatic biliary drainage (PTBD) for malignant distal obstruction when local expertise is available, with recent data reporting technical success around 96.7%.
Therapeutic Interventions and Additional Applications
Two further applications are specific to linear EUS:
- Pseudocyst and pancreatic fluid collection drainage — transmural stents drain fluid collections through the GI wall, with clinical success rates of 70–87% in reviewed series
- Celiac plexus neurolysis (CPN) and block (CPB) — EUS-guided injection of analgesic or neurolytic agents; a 2021 meta-analysis estimated pooled pain relief of approximately 71% for CPN in pancreatic cancer
Linear EUS also characterizes submucosal tumors (GISTs, leiomyomas, carcinoid/neuroendocrine tumors) by identifying the GI wall layer of origin and obtaining tissue via FNB. For mediastinal staging of lung cancer, EUS-FNA through the esophageal wall can sample mediastinal lymph nodes with reported sensitivity of 75% and specificity of 100%.
What to Expect During a Linear EUS Procedure
Preparation
- Fasting: Clear liquids up to 2 hours before; no food for at least 6 hours prior (per ASGE sedation guidance)
- Medications: Anticoagulants (warfarin, clopidogrel) may need to be paused — confirm with the prescribing physician and endoscopy team in advance
- Transportation: Arrange a driver; sedation prevents same-day driving
The Procedure
The patient is positioned on their left side. For upper EUS, a local anesthetic throat spray is applied, then moderate sedation — typically a combination of a benzodiazepine and opioid, or propofol-based — is administered. The linear echoendoscope is introduced through the mouth and advanced to the relevant position.
Procedure duration varies by indication, and therapeutic interventions add time. Plan for a 2–3 hour total visit when accounting for preparation, the procedure itself, and recovery monitoring.
- Diagnostic EUS-FNA (pancreatic mass): median approximately 26 minutes
- Pseudocyst drainage: approximately 24 minutes average
- EUS-guided biliary drainage: typically longer, often 45–70 minutes
Results and Follow-Up
The endosonographer reviews images immediately. If tissue was obtained via FNA or FNB, samples go to a pathologist — results typically return within 3–7 business days. The clinical team will discuss findings and determine next steps, which may include surgical referral, additional imaging, or starting treatment.
Risks, Safety Profile, and Recovery
Safety Overview
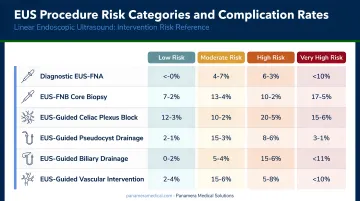
Diagnostic EUS is a low-risk procedure, with reported complication rates of approximately 0.05–0.1%. Risk increases with interventional components. According to ASGE 2022 guidance, post-FNA pancreatitis rates in recent studies were 0.32% and 0.44% — low but clinically relevant figures worth discussing with patients before the procedure.
Specific risks by category:
- Pancreatitis — most associated with FNA of pancreatic tissue
- Bleeding — risk varies by target and needle gauge
- Infection — particularly relevant with cyst aspiration; clinicians may administer prophylactic antibiotics
- Perforation — rare; associated with the esophageal, gastric, or duodenal wall
While serious complications are rare, patients should know which symptoms warrant prompt attention. They should contact their care team or go to an emergency department if they experience:
When to Seek Immediate Care
- Fever or chills after the procedure
- Severe abdominal pain
- Chest or neck pain
- Vomiting blood
- Dark or tarry stools
Recovery
Most patients recover within a few hours at the endoscopy unit and resume normal activities within 24 hours. A mild sore throat is common after upper EUS and typically resolves in 1–2 days. No dietary restrictions apply unless a therapeutic intervention was performed.
Choosing and Sourcing Linear EUS Equipment
What Facilities Should Evaluate
Linear echoendoscopes represent a significant capital investment. Key factors in procurement decisions:
- **Image quality and processor compatibility** — scope-processor pairings must be verified at the model level; published frequency ranges don't substitute for device-specific specs
- Working channel diameter — larger channels (3.7–4.0 mm on current linear models) support a wider range of needles and therapeutic accessories
- Ergonomics — endoscopist comfort affects procedure quality and practitioner sustainability
- Service and parts availability — total cost of ownership includes maintenance, repair turnaround, and technology refresh cycles, not just acquisition price
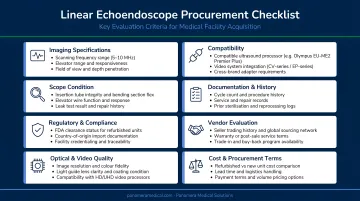
The Olympus GF-UCT180, a curvilinear array echoendoscope operating at 5–12 MHz with a 180° scanning range and 3.7 mm working channel, is a typical example of the linear EUS equipment facilities commonly evaluate today.
Working with a Specialist Trading Partner
Facilities looking to upgrade older-generation linear EUS scopes, trade in existing equipment, or source certified pre-owned echoendoscopes can benefit from working with an experienced specialist rather than navigating the secondary market independently.
Panamera Medical Solutions, with over 15 years of international endoscopy equipment trading experience, offers trade-in and buy-back programs for facilities managing equipment transitions. Older linear EUS scopes that no longer serve a facility's clinical needs retain real value on the secondary market.
Panamera's network spanning North America, Europe, and South America connects that equipment with qualified international buyers. Facilities can apply that value as credit toward newer equipment or convert it to cash.
Whether sourcing through a trade-in or buying outright, Panamera's team can advise on availability, compatibility, and servicing support across major brands including Olympus, Pentax, and Fujifilm.
Frequently Asked Questions
What is a linear endoscopic ultrasound?
Linear EUS is a procedure combining a flexible endoscope with an ultrasound transducer that images in a plane parallel to the scope axis. This orientation enables real-time visualization of structures adjacent to the GI tract and real-time needle guidance for tissue sampling or therapeutic interventions — in a single session.
Are you put to sleep for an endoscopic ultrasound?
Most patients receive moderate sedation — a combination of a sedative and painkiller — rather than full general anesthesia. Some centers use general anesthesia depending on procedure complexity and individual patient factors.
Why would a doctor order an endoscopic ultrasound?
Doctors typically order EUS for one of four reasons:
- Evaluating a lesion or mass found on prior CT, MRI, or standard endoscopy
- Staging cancer with locoregional precision
- Obtaining tissue via FNA or FNB for pathological diagnosis
- Performing therapeutic interventions such as cyst drainage or celiac plexus neurolysis
How long does it take to recover from an endoscopic ultrasound?
Most patients recover within a few hours at the endoscopy unit and can resume normal activities within 24 hours. Patients should not drive on the day of the procedure due to sedation. A mild sore throat may persist for a day or two after upper EUS.
What is the difference between radial and linear EUS?
Radial EUS produces a 360° cross-sectional image and is primarily used for anatomical staging and overview. Linear EUS scans parallel to the scope axis, enabling real-time needle guidance — making it suitable for both diagnosis and therapeutic procedures like biopsy, drainage, and neurolysis.
What conditions can linear EUS diagnose or treat?
Linear EUS covers a broad diagnostic and therapeutic range:
- Pancreatic cancer, pancreatitis, and pancreatic cysts
- Biliary stones and strictures
- GI tract cancers (locoregional staging) and submucosal tumors
- Mediastinal lymph nodes
- Therapeutic applications: pseudocyst drainage and celiac plexus neurolysis for pain management