Introduction
Choosing the wrong endoscope type for a given procedure doesn't just create inconvenience: it can compromise diagnostic accuracy, delay treatment, and expose patients to unnecessary risk. Yet procurement decisions across hospital departments are still often made without a clear framework for when rigid optics are the right call versus when a flexible scope is the only practical option.
The stakes extend beyond the clinical. Equipment budgets, staff training, sterilization infrastructure, and procedure throughput all shift depending on which scope type anchors a department's workflow.
According to MarketsandMarkets, the global endoscopy equipment market is projected to grow from USD $34.83 billion in 2024 to USD $53.54 billion by 2030, reflecting active capital investment across facilities worldwide. With budgets increasingly tied to multi-year procurement cycles, getting scope selection right before a purchase order is signed has real financial consequences.
This guide breaks down the core differences between rigid and flexible endoscopy across design, image quality, sterilization, cost, and clinical use — so procurement managers and clinical leads can match scope type to procedure requirements and justify capital allocation with a clear rationale.
Key Takeaways
- Rigid endoscopes deliver superior precision in surgically accessible cavities — laparoscopy, arthroscopy, and rhinoscopy
- Flexible endoscopes access curved anatomy through natural orifices, making them indispensable for GI and bronchoscopy procedures
- Autoclave sterilization is achievable for most rigid scopes; flexible scopes require more complex high-level disinfection protocols
- Total cost of ownership differs significantly — flexible scopes carry higher acquisition and reprocessing costs
- Most multi-specialty facilities maintain both types to cover their full procedural spectrum
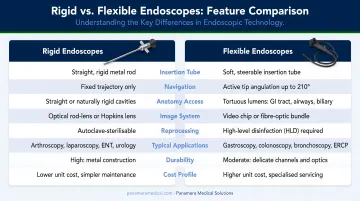
Rigid vs Flexible Endoscopy: Quick Comparison
| Feature | Rigid Endoscopes | Flexible Endoscopes |
|---|---|---|
| Structure | Straight, non-bendable tube | Articulating insertion tube |
| Optics | Rod-lens system | Fiber-optic or video chip (HD/4K) |
| Viewing angles | 0°, 30°, 45°, 70° | Four-way tip deflection |
| Access method | Incision or defined orifice | Natural body orifices |
| Anesthesia | Usually general | Local or sedation |
| Sterilization | Autoclave (most models) | High-level disinfection / chemical sterilization |
| Durability | High; fewer mechanical failure points | Moderate — articulation components wear over time |
| Cost | Lower upfront; lower maintenance | Higher upfront; more costly to repair |
Design & Structure
Rigid endoscopes use a straight, non-bendable shaft with a rod-lens optical system. Karl Storz's HOPKINS telescopes and Olympus rigid laparoscopes are available in diameters from 2.7 mm to 10 mm, with viewing angles at 0°, 30°, 45°, and 70° depending on model and application.
Flexible endoscopes use an articulating insertion tube with four-way distal tip deflection. The Olympus CF-HQ190L colonoscope, for example, achieves 180° up, 180° down, 160° right, and 160° left angulation — essential for navigating the colon's curvature.
Image Quality
Rod-lens technology in rigid scopes delivers high brightness, contrast, and resolution. The Royal College of Surgeons notes the Hopkins rod-lens system provided a fifty-fold improvement in light transmission over earlier designs.
A peer-reviewed optical study of a 4 mm ultra-high-definition arthroscope measured 22.3 line pairs/mm resolution — a benchmark that illustrates the optical ceiling modern rigid scopes can reach in surgical settings.
Flexible video endoscopes have narrowed that optical gap in recent years. Pentax's i20c platform supports up to 4K resolution with a compatible processor, and Fujifilm's ELUXEO 800 series uses CMOS sensors with image-enhanced endoscopy modes. For luminal GI procedures, flexible scopes now offer imaging that meets clinical needs; for joint or sinus work, rigid optics still tend to be the preferred choice.
What Is Rigid Endoscopy?
A rigid endoscope is a straight, non-flexible visualization instrument built around a rod-lens optical system. Light travels through the rigid shaft along a fixed trajectory, producing high-resolution images within a defined anatomical space — typically accessed through a small surgical incision or a specific natural opening.
Core Components
A complete rigid endoscope setup includes:
- Rigid telescope: available in 0°–70° viewing angles; 2.7 mm and 4–5 mm diameters are most common in surgical practice
- Light source and cable to deliver illumination through the shaft
- Video camera at the eyepiece, connected to a monitor for real-time visualization
- Operative sheaths for biopsy forceps, scissors, or graspers — swappable without removing the scope
That swappable sheath design matters in the OR: it allows surgeons to change instruments mid-procedure without withdrawing and reinserting the scope, saving time and reducing tissue disruption.
Clinical Advantages
Rigid scopes bring several strengths to the operating environment:
- Superior optical clarity and depth of field in confined surgical cavities
- Mechanical stability that supports precise instrument manipulation
- Autoclave sterilization compatibility (verify per the manufacturer's IFU for each model)
- Olympus Goldtip rigid laparoscopes carry a five-year warranty against autoclave damage, reflecting the durability expectation built into the design
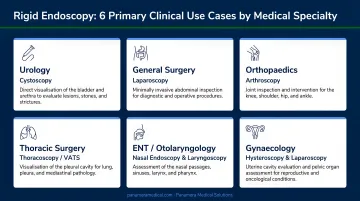
Use Cases of Rigid Endoscopy
Rigid endoscopes are the standard of care across several specialties:
- Laparoscopy — abdominal organ visualization, biopsy, staging of selected cancers; SAGES guidelines support its use for acute abdominal pain, chronic pelvic pain, and trauma evaluation
- Arthroscopy — joint examination and repair; an estimated 1.77 million surgical arthroscopy procedures are performed annually in the United States
- Rhinoscopy/sinus surgery — nasal cavity visualization in ENT procedures
- Cystoscopy/urethroscopy — bladder and urethral surveillance, especially in bladder cancer monitoring
- Thoracoscopy — minimally invasive chest cavity examination
- Neurosurgery — ventricular access and intracranial visualization
Across these specialties, rigid scopes are the go-to when procedures demand multi-instrument access, mechanical force, or the highest optical precision within a surgically accessible cavity — requirements that flexible alternatives simply can't match in these contexts.
What Is Flexible Endoscopy?
Flexible endoscopy uses a steerable insertion tube that navigates bends, curves, and the full length of the body's luminal pathways. Modern flexible endoscopes transmit images via either fiber-optic bundles or a CCD/CMOS chip positioned at the distal tip, sending real-time video to an external monitor.
Core Components
- Flexible insertion tube — four-way angulation capability; the Olympus GIF-HQ190 gastroscope achieves 210° upward deflection
- Working/accessory channel — typically 2.8 mm to 3.7 mm in diameter; enables passage of biopsy forceps, snares, stents, and retrieval tools
- Air/water flushing and suction — maintains a clear visual field and removes debris
- Control handle — designed for single-operator scope manipulation throughout the procedure
The working channel is where diagnostic capability meets therapeutic action. A single scope insertion can combine visualization, biopsy, and treatment in one session.
Clinical Advantages
- Traverses tortuous anatomy physically inaccessible to a rigid tube
- Accesses most GI and airway sites through natural orifices, with no surgical incision required
- Real-time video output viewable by the entire operative team
- Compatible with a wide accessory ecosystem: biopsy forceps, polypectomy snares, dilation balloons, stents
Use Cases of Flexible Endoscopy
Flexible endoscopy handles a large portion of global diagnostic volume. ASGE reports 22,162,641 GI endoscopic procedures were performed in the U.S. in 2019 alone — including 13.8 million colonoscopies and 7.4 million upper endoscopies.
Key applications include:
- Upper GI endoscopy (gastroscopy/esophagoscopy) — diagnosis of gastritis, IBD, Barrett's esophagus, and GI neoplasia
- Colonoscopy — colorectal cancer screening; USPSTF recommends colonoscopy every 10 years for average-risk adults aged 45–75
- Bronchoscopy — airway and lung assessment for hemoptysis, suspected tumors, infection, and foreign body retrieval
- Therapeutic procedures — polypectomy, hemostasis, stent placement, and ERCP
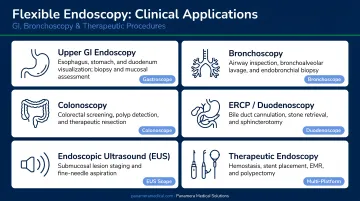
Current ESGE guidelines support cold snare polypectomy for small colorectal polyps (2024) and covered metal stents for malignant dysphagia (2021) — both performed through a flexible scope without a separate surgical session.
For procurement teams, this breadth of application means a single flexible endoscope model can support multiple departments — making per-procedure cost and scope utilization rate key metrics when evaluating equipment investments.
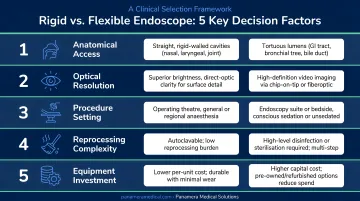
Rigid vs Flexible Endoscopy: Which Is Right for Your Facility?
No single scope type wins across every scenario. The right decision comes down to five factors:
- Target anatomy — Is the area accessible via a natural orifice, or does it require surgical entry?
- Procedure requirements — Does the task demand high mechanical precision, or the ability to navigate curves?
- Patient population — What's the tolerance for general anesthesia versus sedation or local anesthetic?
- Sterilization infrastructure — Does the facility have AER capacity and HLD protocols, or is autoclave-based processing the norm?
- Total cost of ownership — A 2025 NHS micro-costing study estimated reusable GI endoscopy at approximately £107 per procedure (roughly $135 USD), with capital acquisition accounting for £46.90 of that figure. Though UK-specific, these figures offer a useful modeling benchmark for US facilities comparing reusable versus disposable scope economics
When to Choose Rigid
- Joint surgery, laparoscopic biopsy, or sinus procedures requiring optical precision in a defined cavity
- High-volume departments in a single anatomical specialty (orthopedics, urology, ENT)
- Facilities where autoclave sterilization is the standard workflow and HLD infrastructure is limited
When to Choose Flexible
- GI endoscopy, bronchoscopy, or any procedure traversing long luminal structures
- Clinical settings where the same scope session must handle both diagnosis and therapy (biopsy + polypectomy, visualization + stenting)
- Patient populations where minimizing anesthesia exposure is a clinical priority
Operating Both Types
Most hospitals and multi-specialty clinics run both. The practical approach is to map scope type to service line volume — rigid scopes anchored to surgical and specialty departments, flexible scopes handling the GI and pulmonary workflow. Done well, that mapping prevents redundant capital expenditure and gives procurement teams a defensible basis for future equipment decisions.
Facilities looking to rebalance their equipment mix without full capital outlay can explore trade-in and buy-back options. Panamera Medical Solutions specializes in sourcing, valuing, and trading flexible endoscopic equipment globally — covering Olympus, Pentax, Fujifilm, Karl Storz, and Stryker platforms across North America, Europe, and South America. Their buy-back program lets facilities apply credit toward newer equipment or liquidate underutilized scopes, which can offset transition costs when shifting service lines or replacing aging inventory.
Conclusion
Neither rigid nor flexible endoscopy holds universal superiority. The right scope for any procedure is determined by anatomy, clinical task, patient need, and operational reality.
Two decision triggers cut through the complexity: if you need precision and mechanical stability in a defined surgical cavity, rigid optics are the stronger choice. If you need reach, maneuverability, and minimal patient invasiveness through luminal pathways, flexible is the only viable option.
Getting this right has measurable downstream effects on operations and outcomes:
- Procedure times shorten with the right tool for the anatomy
- Diagnostic yield improves when scope reach and optics match the task
- Sterilization workflows simplify when scope type aligns with reprocessing capacity
- Long-term maintenance costs stay manageable with appropriate equipment selection
These show up directly in quality metrics, budget reviews, and patient outcome data.
For facilities navigating an equipment upgrade or rationalizing an existing mix, scope selection decisions carry long-term cost implications — making it worthwhile to evaluate trade-in value, reprocessing compatibility, and procedural fit before committing to new inventory.
Frequently Asked Questions
What is the difference between rigid esophagoscopy and flexible esophagoscopy?
Rigid esophagoscopy uses a straight metal tube, performed in the OR under general anesthesia, and delivers superior optics for precise interventions like foreign body removal or stricture dilation. Flexible esophagoscopy uses a steerable scope under sedation or topical anesthesia, offering better patient comfort and real-time video imaging through the natural curves of the esophagus.
Is flexible endoscopy painful?
Flexible endoscopy is generally not painful. Patients receive local anesthesia, sedation, or a combination, and ASGE guidelines call for sedation titrated to each patient's comfort and safety. Mild discomfort such as pressure or bloating may occur, but the flexible design minimizes tissue trauma.
Can an endoscopy detect liver cirrhosis?
Endoscopy does not directly diagnose liver cirrhosis. However, upper GI flexible endoscopy can identify complications of cirrhosis, such as esophageal varices and portal hypertensive gastropathy. Diagnosing cirrhosis itself requires imaging, laboratory testing, or liver biopsy.
Which endoscope type is easier to sterilize?
Rigid endoscopes are generally easier to sterilize; most can withstand steam autoclave processing. Flexible endoscopes require high-level disinfection or chemical sterilization due to heat-sensitive internal components, making reprocessing more demanding and costly overall.
What medical specialties most commonly use rigid endoscopes?
Rigid endoscopes are standard in orthopedic surgery (arthroscopy), urology (cystoscopy), laparoscopic and general surgery, ENT (rhinoscopy, laryngoscopy), neurosurgery, and gynecology: specialties where precise visualization in a defined anatomical cavity is essential.
How long do rigid and flexible endoscopes typically last before needing replacement?
Rigid endoscopes are mechanically durable and can last well beyond a decade with proper care; Olympus, for example, provides a five-year autoclave warranty on its Goldtip rigid laparoscopes. Flexible endoscopes have a shorter lifespan due to wear on moving parts and internal channels, with the NHS assuming a seven-year capital lifespan as a standard planning benchmark.