For GI facilities, endoscopy reprocessing staff, and equipment managers, understanding why contamination happens is the first step toward preventing it. This article breaks down the root causes, the consequences of inaction, and the layered prevention strategies that actually work.
Key Takeaways
- Duodenoscope elevator mechanisms create crevices where bacteria survive even after high-level disinfection
- Manual pre-cleaning failure is the single most preventable cause of persistent contamination
- MDR organisms including CRE and Pseudomonas aeruginosa have caused patient deaths linked to contaminated ERCP scopes
- Culturing sensitivity ranges from 82.2% to 98.9%; one negative result cannot clear a quarantined scope
- Prevention requires layered controls: rigorous cleaning, surveillance culturing, staff training, and timely equipment upgrades
Common Causes of ERCP Scope Contamination
ERCP scope contamination occurs when biological material — tissue, fluid, or bacteria — from one patient persists on or inside the scope after reprocessing and transfers to the next patient. That definition sounds straightforward, but the causes rarely are.
Contamination in duodenoscopes typically results from a combination of factors: the scope's physical design, reprocessing technique, and protocol gaps. Identifying the specific cause matters because the corrective action differs for each one.
Complex Scope Design and Hard-to-Clean Components
The elevator mechanism at the distal tip of a duodenoscope steers guidewires and accessories into the bile duct, making ERCP possible. It also creates the scope's biggest infection control liability.
The elevator's tight crevices and mechanical joints are inaccessible to standard brushes. Organic debris accumulates in these recesses during a procedure, and even after high-level disinfection (HLD), residual contamination persists.
Research by Li et al. (2024) found peak bioburden in the elevator recess reaching 9.15 × 10⁸ CFU/piece after clinical use — with 7.14% of post-HLD samples still testing positive.
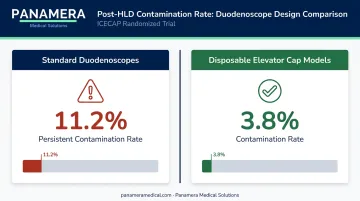
The ICECAP randomized trial reinforced this: standard duodenoscopes showed 11.2% persistent contamination after HLD, compared to 3.8% for disposable elevator cap models.
Inadequate Manual Pre-Cleaning
Manual pre-cleaning — the bedside and reprocessing room steps performed before HLD — is the most critical stage in the entire reprocessing sequence. If organic material remains on the scope, disinfectants cannot penetrate to the bacteria underneath. No AER compensates for a poorly cleaned scope.
This step fails in predictable ways:
- Rushed bedside wipe-down without flushing all channels
- Staff who received awareness training but not hands-on competency assessment
- Inconsistent brushing technique in narrow working channels
- Failure to actuate the elevator during cleaning — leaving the recess untouched
Okamoto et al. (2022) found that 27.7% of reprocessing reviews identified protocol deviations, with failure to flush the elevator recess or move the elevator during cleaning among the most common.
Failures in High-Level Disinfection or Sterilization
Even when manual cleaning is adequate, errors at the HLD stage allow pathogens to survive. Common failure points include:
- Incorrect disinfectant concentration or expired chemical solution
- Inadequate soak time or temperature
- AER malfunction not caught through routine validation
- Skipping enhanced sterilization steps for immunocompromised patients
Beyond procedural errors, certain MDR organisms can survive even correctly performed HLD. Research by Kwakman et al. (2022) found Pseudomonas aeruginosa persisting in duodenoscope channels after HLD in a controlled setting. The FDA issued its first duodenoscope safety communication in February 2015 specifically because standard reprocessing instructions were insufficient to prevent CRE transmission.
Equipment Wear, Aging, and Damage
Physical deterioration compounds every other contamination risk. Micro-cracks, worn seals, and degraded channel walls create harboring sites for bacteria and biofilm that no cleaning protocol can reach, and many of these defects are invisible during routine inspection.
The multisociety reprocessing guideline notes that two documented contamination events were directly linked to unexpected wear or vendor-identified repair needs, even when the scopes had passed local functional assessments.
Okamoto et al. found high-concern organism contamination of 6.6% in older TJF-160F/VF models versus 4.1% in newer TJF-Q180V models — a gap that grows as instruments accumulate additional wear cycles.
What Happens If ERCP Scope Contamination Is Ignored
Patient Safety Consequences
The primary harm is transmission of MDR organisms between patients. CRE, MRSA, and Pseudomonas aeruginosa are particularly dangerous for the immunocompromised and critically ill patients who most commonly undergo ERCP. These infections can progress to sepsis and death.
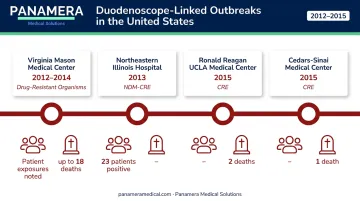
The documented US outbreak record makes this concrete:
| Facility | Year | Pathogen | Impact |
|---|---|---|---|
| Northeastern Illinois Hospital | 2013 | NDM-producing CRE | 44 patients identified; 23 of 50 tested positive |
| Ronald Reagan UCLA Medical Center | 2015 | CRE | 179 exposed; 7 infected; 2 deaths |
| Cedars-Sinai Medical Center | 2015 | CRE | 67 exposed; 4 infected; 1 death |
| Virginia Mason Medical Center | 2012–2014 | Drug-resistant organisms | 32–39 infected; 11–18 deaths among infected |
The CDC MMWR report on the Illinois outbreak found that 75% of confirmed case-patients had undergone ERCP at the implicated hospital, versus only 4% of controls — a stark illustration of scope-to-patient transmission.
Operational and Regulatory Consequences
Beyond patient harm, an uncontrolled contamination event sets off a chain of institutional consequences that are difficult to contain:
- Immediate scope quarantine and procedure cancellations
- Mandatory FDA medical device reporting
- Potential regulatory investigation and facility audit
- Legal liability and reputational damage that erodes patient and referral trust
Warning Signs to Watch For
Contamination problems rarely announce themselves with obvious signs. These early indicators often precede an outbreak:
- Surveillance cultures turning positive — especially intermittently, with false-negative results in between
- Unexplained post-ERCP fevers or septicemia — particularly when the causative organism matches GI flora
- Visible scope deterioration — cracked channels, stiff elevator mechanisms, compromised seals, or failed leak tests that suggest reprocessing gaps
Any of these warrants immediate scope quarantine and a full root-cause investigation — delays increase exposure risk for every subsequent patient.
How to Prevent ERCP Scope Contamination
No single measure eliminates contamination risk. Effective control requires layering multiple interventions — each one catching failures the others might miss.
Rigorous Manual Pre-Cleaning at the Point of Use
Immediately after each ERCP, bedside pre-cleaning should include:
- Wipe the insertion tube with an enzymatic detergent cloth
- Flush all channels with enzymatic solution
- Actuate the elevator to expose the recess for cleaning
Full manual cleaning in the reprocessing room — per the manufacturer's validated sequence — must follow before the scope enters the AER. This step physically removes the organic load that would shield bacteria from disinfectants. There is no substitute.
Microbiological Surveillance Culturing
Regular culturing provides the only available method to detect residual contamination after reprocessing. The FDA/CDC/ASM standardized Duodenoscope Surveillance Sampling and Culturing Protocol specifies sampling from:
- The instrument (biopsy) channel
- The elevator recess
- The elevator wire channel (on applicable models)
- Seams at the distal cap
Any scope yielding a positive result should be quarantined immediately.
One critical limitation: culturing is not perfect. Van der Ploeg et al. (2025) estimated current culturing sensitivity at 82.2% to 98.9%, and found that 12.3% to 23.7% of ERCP procedures may have been performed with contaminated scopes under study assumptions. A single negative culture should not be used as the sole criterion to release a quarantined scope.
Transitioning to Newer-Generation or Single-Use Scope Designs
The FDA recommended in August 2019 that facilities begin transitioning away from older fixed-endcap duodenoscopes. The clinical data supports this: older fixed-endcap models showed 4–6% high-concern organism contamination in FDA postmarket surveillance, while the Fujifilm ED-580XT achieved 1.1% in the same studies.
For facilities evaluating their duodenoscope inventory, the transition does not require a full capital outlay at once. Trade-in and buy-back programs — such as those available through Panamera Medical Solutions — allow facilities to retire older Olympus or Pentax duodenoscopes and apply their residual value toward newer-generation models like the Olympus TJF-Q190V or Pentax ED34-i10T2.
Depending on the arrangement, residual value applies as credit toward replacement equipment or as a cash buyout of decommissioned inventory.
Strict Protocol Compliance and Reprocessing Staff Training
Human error is a consistent contributor to reprocessing failures, and awareness training alone does not eliminate it. Effective programs include:
- Written SOPs covering every step of the reprocessing sequence
- Competency-based training with hands-on assessment (not just annual sign-offs)
- Regular reprocessing unit audits — AER validation, chemical concentration checks, documentation reviews
- A designated infection control liaison for endoscopy reprocessing who tracks protocol updates
Standardized workflows close the gaps that individual variation — whether from inexperience or time pressure — consistently opens.
Tips for Long-Term Prevention and Control
Sustained contamination control extends beyond the reprocessing room. These practices reinforce the system over time:
- Conduct leak tests before every reprocessing cycle and send scopes for manufacturer servicing at defined intervals — retire instruments showing signs of internal damage or excessive wear rather than continuing to use them
- Centralize documentation of all culture results, reprocessing logs, and scope usage data to spot trends — a scope that repeatedly yields positive cultures is a retirement candidate, not a candidate for continued diagnostic use
- Keep reprocessing staff current on evolving FDA safety communications and updated manufacturer reprocessing instructions; assign a designated liaison to track these changes
- Plan equipment replacements proactively — retiring aging duodenoscopes on schedule eliminates the risk that deteriorating scopes present to patients and the facility's regulatory standing
Conclusion
ERCP scope contamination has clear, documented causes — design complexity, pre-cleaning failures, protocol gaps, and equipment aging — and each one is addressable.
Effective prevention is layered:
- Consistent, complete manual pre-cleaning at every procedure
- Validated disinfection protocols and AER oversight
- Regular microbiological surveillance with appropriate scope quarantine
- Timely transitions to newer-generation equipment with lower inherent contamination risk
Proactive contamination control protects patients, prevents procedure shutdowns, and keeps facilities on the right side of regulatory scrutiny. The 2013–2015 outbreak clusters showed exactly what happens when reprocessing gaps go unaddressed — patient harm, facility investigations, and significant operational disruption. Facilities that treat scope hygiene as an ongoing operational priority, not a reactive checklist item, are the ones that avoid those outcomes.
Frequently Asked Questions
How do you clean an ERCP scope?
ERCP scope cleaning begins with immediate bedside pre-cleaning — wiping the insertion tube, flushing all channels with enzymatic detergent, and actuating the elevator. Full manual cleaning follows in the reprocessing room, including brushing all channels and the elevator recess, before the scope undergoes high-level disinfection or sterilization in an Automated Endoscope Reprocessor per the manufacturer's validated instructions.
Can you get a bacterial infection from an endoscopy?
While rare, bacterial infections can be transmitted through improperly reprocessed endoscopes. ERCP scopes carry the highest documented risk due to their complex elevator mechanism, and MDR organism outbreaks (including CRE transmissions causing patient deaths) have been linked to contaminated duodenoscopes even when standard cleaning instructions were followed.
Is ERCP a high-risk procedure?
ERCP carries inherent procedural risks including pancreatitis (roughly 8% of average-risk cases per ASGE guidelines), bleeding, and perforation, separate from scope-related infection risk. With proper reprocessing, scope-related infection risk is substantially reduced, and ERCP remains a clinically essential procedure for serious pancreatic and biliary conditions.
What bacteria are most commonly found on contaminated ERCP scopes?
Common organisms include gut and oral flora, alongside high-concern pathogens such as Pseudomonas aeruginosa, carbapenem-resistant Enterobacteriaceae (CRE), and other MDR organisms. These pathogens are particularly dangerous for immunocompromised ERCP patients, who often have limited capacity to fight serious secondary infections.
How reliable is microbiological culturing for detecting contaminated duodenoscopes?
Culturing is the only available detection method but has known limitations: Van der Ploeg et al. estimated sensitivity at 82.2% to 98.9%, meaning false negatives can occur. A single negative result should not automatically clear a quarantined scope, particularly one with prior positive cultures or visible wear.
When should a duodenoscope be taken out of service?
A scope should be quarantined immediately upon a positive culture result, failed leak test, visible physical damage, or suspected link to a patient infection. Retirement should be considered when a scope repeatedly yields positive cultures, shows wear that compromises cleanable surfaces, or fails functional assessment.