Key Takeaways
- ERCP scope diameter refers to three distinct measurements: tip outer diameter (OD), insertion tube OD, and instrument channel internal diameter (ID)
- Standard therapeutic adult duodenoscopes have a 13+ mm tip OD and 4.2 mm instrument channel ID: the benchmarks for therapeutic ERCP
- The instrument channel ID is the primary constraint on accessory selection — stents, guide wires, and sphincterotomes must be matched to this dimension
- Device-assisted enteroscopes carry 2.8–3.2 mm channels, restricting stent and accessory options
- Used or refurbished scopes require dimensional verification; channel wear and elevator damage can reduce effective clearance below rated spec
What ERCP Scope Diameter Represents
Three distinct dimensional parameters define an ERCP scope — and each one governs a different aspect of the procedure.
The Three Dimensions
| Parameter | What It Controls |
|---|---|
| Insertion tube OD | Patient passage through the pharynx and esophagus; sedation requirements |
| Distal tip OD | Intubation feasibility — especially at the pylorus and in restricted anatomy |
| Instrument channel ID | The upper bound on every accessory used during the procedure |
The FDA/CDC duodenoscope surveillance protocol defines the instrument channel as the passage from biopsy port to distal end through which accessories — guide wires, sphincterotomes, forceps — are inserted. The distal tip is defined separately and includes the elevator lever and elevator recess. In this guide, OD refers to outer diameter and ID to inner diameter throughout.
The French Sizing Connection
Accessories are sized in French units (1 Fr = 0.33 mm). A 10 Fr stent has an OD of approximately 3.3 mm. The instrument channel ID must comfortably exceed that figure to allow controlled passage, contrast injection, and wire manipulation without jamming.
Both figures — channel ID and accessory OD — must be confirmed before the procedure, not assumed from model familiarity alone.
The Elevator Adds a Third Constraint
The forceps elevator — the pivoting mechanism unique to side-viewing duodenoscopes — sits at the instrument channel outlet. When raised, it deflects accessories by up to nearly 90 degrees. That geometry introduces an additional compatibility constraint beyond simple channel diameter: the elevator angle and channel exit geometry interact with accessory OD to affect deflection range and insertion resistance.
Forcing an oversized accessory through a tight channel risks elevator mechanism damage, accessory fracture, and loss of deflection control mid-procedure — none of which are recoverable without scope withdrawal.
Standard Diameter Ranges Across ERCP Scope Types
Diameter specs vary meaningfully across the three scope categories used in ERCP. Here's what the verified manufacturer data shows.
Standard Therapeutic Adult Duodenoscopes
| Model | Tip OD | Insertion Tube OD | Channel ID |
|---|---|---|---|
| Olympus TJF-Q190V | 13.5 mm | 11.3 mm | 4.2 mm |
| Fujifilm ED-580XT | 13.1 mm | 11.3 mm | 4.2 mm |
The 4.2 mm channel is the established benchmark for therapeutic ERCP. It accommodates sphincterotomes, 10–11.5 Fr plastic stents, stone extraction baskets and balloons, and cholangioscope systems designed for this channel size.
The TJF-Q190V's widespread adoption makes it one of the most actively sourced duodenoscopes in the pre-owned market, which matters for facilities managing equipment lifecycle costs.
Pediatric Duodenoscope
The Olympus PJF-160 pediatric duodenoscope carries a 7.5 mm tip OD, a 7.5 mm insertion tube OD, and a 2.0 mm instrument channel — dimensions confirmed in peer-reviewed literature from 2019 and 2024. Olympus has discontinued the PJF-160, but equivalent designs remain relevant for:
- Infants under 12 months
- Patients weighing less than 10–12 kg
- Cases with anatomical restriction where adult scope geometry fails
The adult therapeutic duodenoscope is generally safe and effective for children older than 12 months weighing more than 10 kg. For patients below those thresholds, the pediatric instrument becomes necessary — not optional.
Device-Assisted Enteroscopes (Surgically Altered Anatomy)
| Model | Channel ID | Insertion Tube OD | Max Stent Supported |
|---|---|---|---|
| Olympus SIF-Q180 (SBE) | 2.8 mm | 9.2 mm | 7 Fr (with constrainer) |
| Olympus SIF-H290S (short SBE) | 3.2 mm | 9.2 mm | 8.5 Fr |
| Fujifilm EN-580T (DBE) | 3.2 mm | 9.3 mm | 8.5 Fr |
WEO guidance on device-assisted ERCP notes that 7 Fr stents can be passed through 2.8 mm channels but may require a stent constrainer to prevent flap jamming. The newer 3.2 mm double-balloon enteroscopes support 8.5 Fr stents, a real gain over 2.8 mm systems, though capacity still falls well short of what a standard therapeutic duodenoscope provides.
How Diameter Governs Accessory and Clinical Compatibility
Every accessory used in ERCP has a published OD that must be matched to the scope's channel ID. This is where dimensional mismatches become procedural problems.
Guide Wire Compatibility
ERCP guide wires range from 0.018 to 0.035 inches. The 0.035-inch wire is standard for most therapeutic applications through a 4.2 mm channel. Compatibility isn't just scope-to-wire, though — wire diameter must also match the lumen of the sphincterotome being used. That's two compatibility checks before the procedure begins.
Stent Sizing: What Each Channel Can Support
According to a peer-reviewed biliary stenting review and verified manufacturer specifications:
- 7 Fr stents — require 3.2 mm channel minimum (Boston Scientific Advanix)
- 8.5 Fr stents — require 3.2 mm channel minimum
- 10 Fr stents — require 3.7 mm channel (Cook ST-2) or 4.2 mm (Boston Scientific Advanix, depending on delivery system)
- 11.5 Fr stents — require 4.2 mm channel across all major systems
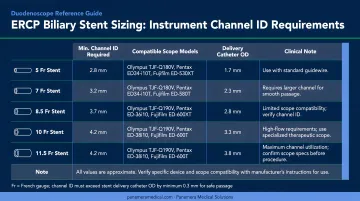
The 10 Fr plastic stent is the most commonly placed biliary stent, which is one reason the 4.2 mm channel carries such clinical weight. In device-assisted ERCP through a 2.8 mm enteroscope, achieving adequate biliary drainage often requires multiple sequential 7 Fr insertions — a real procedural constraint.
Self-Expanding Metal Stents
Where plastic stents follow relatively predictable sizing rules, SEMS introduce a separate variable: the delivery catheter. Its OD must be verified against the scope's channel ID independently of the stent itself.
In older or non-standard scope models, channel wear may have reduced effective internal clearance below the nominal rated value. Always verify clearance against the actual datasheet before the procedure — don't rely on the nominal spec alone.
Sphincterotome Fit
The sphincterotome's bowing mechanism — tension on the cutting wire — changes the device's effective cross-section at the elevator exit. A tight channel fit restricts bowing range, which directly impairs cannulation angle. This is one reason a scope that is nominally compatible by channel ID alone may still present handling problems in practice.
How ERCP Scope Diameter Is Specified and Verified
Manufacturer Documentation
Olympus and Fujifilm publish separate specification fields for distal tip OD, insertion tube OD, and instrument channel ID in their datasheets. These are the most directly verifiable procurement fields and should be the first reference point when selecting or evaluating a scope.
FDA 510(k) clearances — such as K220587 for the Olympus TJF-Q190V — include nonclinical verification and validation categories, though public summaries typically do not expose numeric manufacturing tolerances for individual dimensions.
Field Verification Limitations
Formal dimensional measurement (bore gauges, acceptance-test tooling) is a manufacturing and repair-lab activity. In clinical settings, field indicators include:
- Cleaning brush resistance — brushes are sized to channel ID spec; poor passage suggests debris accumulation or channel damage
- Accessory insertion resistance — unexpected resistance may indicate reduced effective clearance
- Visual inspection at the elevator recess — the most reprocessing-sensitive area on the scope

The CDC and ASGE both direct facilities to perform thorough manual cleaning consistent with the manufacturer's IFU, including brushing and flushing all channels. The 2021 ASGE multisociety reprocessing guideline is the current reference standard for this process.
Lifecycle Degradation
An FDA recall for the Olympus TJF-Q190V (initiated July 2023) requires annual inspections of the forceps elevator mechanism or every 100 reprocessing cycles. This reflects a documented reality: repeated reprocessing cycles degrade channel and elevator integrity over time.
Clinical evidence reinforces this concern. A 2023 randomized clinical trial found that disposable elevator-cap duodenoscopes showed reduced contamination after high-level disinfection compared with standard reusable designs, confirming that the elevator recess is the highest-risk structural point on these instruments.
Operating Outside Spec: Consequences and Misinterpretations
Accessory Incompatibility
Using a scope whose channel ID is smaller than the accessory requires forces a hard stop: the accessory won't pass, or won't pass safely. Attempting to force an oversized device risks elevator mechanism damage (a known failure point) and creates debris accumulation in the elevator recess that compounds reprocessing difficulty. Both Fujifilm and Boston Scientific explicitly warn against forcing accessories through the working channel if resistance is encountered.
Patient-Side Risks from Tip OD Mismatch
A tip OD that is too large for the patient's anatomy causes mucosal trauma, failed intubation, or procedural abandonment. The SAGES pediatric ERCP abstract documents exactly this scenario: a 17-month-old patient with an anomalous lower esophageal sphincter where the adult duodenoscope (13 mm tip) could not be negotiated, requiring the pediatric scope instead. This is a clinical decision with a dimensional root cause.
An FDA Class 2 recall for the Olympus TJF-Q190V also links mucosal injuries in the esophagus, stomach, and duodenum to the forceps elevator region and distal cover, confirming that the distal tip geometry carries patient-safety implications beyond instrument channel sizing alone.
Two Persistent Misinterpretations
**1. Channel ID as the only dimension that matters. Tip OD and insertion tube OD determine whether the scope can reach the target anatomy at all. A scope with the correct 4.2 mm channel but an incompatible tip OD for a given patient is still the wrong scope for that case.
**2. "Therapeutic" as a dimensional guarantee. Older therapeutic models, device-assisted scopes, and some non-OEM refurbished units may carry different channel IDs. Verified channel IDs across the ERCP scope spectrum range from 2.0 mm (Olympus PJF-160) to 4.2 mm (adult therapeutic models). "Therapeutic" is a label, not a specification.
Used and Refurbished Scopes: What This Means for Procurement
When sourcing used duodenoscopes, lab-specified dimensions from a datasheet do not automatically reflect in-service condition. A MAUDE report from May 2024 involving an Olympus TJF-Q190V describes a small tear discovered in the inner sheath during borescope inspection, with no clear indication of when the tear occurred or its cause. Channel integrity, reprocessing history, and elevator mechanism condition all require direct assessment before a unit enters clinical use.
Panamera Medical Solutions handles the TJF-Q190V and the Pentax ED34-i10T2 through its trade-in and resale programs, evaluating each unit's full dimensional profile — channel ID, tip OD, and elevator condition — before resale. For facilities managing mixed caseloads (standard adult, altered-anatomy, or pediatric), that full-profile assessment matters more than the nominal channel ID in a catalog.
Frequently Asked Questions
What is the diameter of an ERCP scope?
Diameter covers three separate measurements. For the standard therapeutic adult duodenoscope, the tip OD is approximately 13–13.5 mm, the insertion tube OD is around 11.3 mm, and the instrument channel ID is 4.2 mm. These figures vary by manufacturer and model.
What kind of scope is used for ERCP?
The standard ERCP scope is a side-viewing therapeutic duodenoscope, which differs from forward-viewing gastroscopes in optics orientation and includes a forceps elevator mechanism. In patients with surgically altered anatomy (Roux-en-Y, Whipple), single- or double-balloon enteroscopes are used instead.
What is the instrument channel diameter of a standard duodenoscope?
The standard therapeutic adult duodenoscope has a 4.2 mm instrument channel ID. This dimension determines which guide wires, sphincterotomes, stents, and retrieval devices can pass through the scope.
How does ERCP scope diameter differ between adult and pediatric patients?
The adult therapeutic duodenoscope (tip OD ~13 mm) is used in most pediatric patients over 12 months and above approximately 10 kg. The pediatric duodenoscope (tip OD ~7.5 mm, channel ID 2.0 mm) is reserved for cases with anatomical restriction. The trade-off is a significantly narrower working channel that limits therapeutic capability.
Does ERCP scope diameter affect accessory compatibility?
Directly. The instrument channel ID sets a hard upper limit on accessory size. A 4.2 mm channel supports 10–11.5 Fr stents and 0.035-inch guide wires; a 2.8 mm enteroscope channel restricts stents to 7 Fr. Compatibility must be verified at both the scope level and the individual accessory level before the procedure.
Is ERCP uncomfortable for patients?
ERCP is performed under conscious sedation or general anesthesia. The therapeutic duodenoscope's larger tip OD, compared to a standard diagnostic gastroscope, makes adequate sedation especially important, particularly in patients where scope diameter and anatomy interact closely.