What Is Endobronchial Ultrasound (EBUS)?
Endobronchial ultrasound is a minimally invasive diagnostic technique that combines bronchoscopy with real-time ultrasound imaging. It allows clinicians to visualize the airway wall, surrounding mediastinal structures, and adjacent lymph nodes — without open surgery or surgical incision.
EBUS technology developed in two key stages:
- 1992 — Hurter et al. described radial probe ultrasound for airway use, with 20–30 MHz miniprobes capable of 360-degree imaging
- 2002–2004 — Convex probe EBUS (CP-EBUS) entered clinical practice with real-time needle aspiration; Yasufuku et al. published the foundational description of a 7.5 MHz convex probe scanning parallel to the bronchoscope's insertion axis
Today, EBUS is performed by interventional pulmonologists in dedicated bronchoscopy suites, often as an outpatient procedure. It has become embedded in clinical guidelines from the ERS/ESGE/ESTS for lung cancer mediastinal staging and from the American Thoracic Society for sarcoidosis, given its high diagnostic yield, low complication rate, and outpatient feasibility.
Key Takeaways
- EBUS combines bronchoscopy with real-time ultrasound to sample mediastinal and hilar structures without surgery
- Two probe types exist — radial (RP-EBUS) and convex (CP-EBUS) — with distinct clinical roles
- EBUS-TBNA is the preferred first-line procedure for NSCLC staging, sarcoidosis, and mediastinal lymphadenopathy
- Complication rates stay under 1.5% across large registries, making EBUS well-suited for outpatient settings
- At least 3 passes per lymph node are recommended without ROSE
- Molecular testing requires 4 or more passes per node to yield adequate material
Types of EBUS: Radial Probe vs. Convex Probe
Radial Probe EBUS (RP-EBUS)
RP-EBUS uses miniature ultrasound probes operating at 20–30 MHz, producing a 360-degree radial image of the airway wall and surrounding tissue with penetration depth of approximately 4–5 cm. The ultra-miniature versions (around 1.7 mm OD) fit through a guide sheath into peripheral airways.
Key strengths:
- Visualizes peripheral pulmonary nodules beyond standard bronchoscopic reach
- Distinguishes airway infiltration from external compression
- Useful for mapping the relationship between lesions and surrounding vasculature
Key limitation:
- Does not allow real-time biopsy — tissue sampling requires a guide sheath-assisted approach after probe withdrawal, reducing targeting precision compared to CP-EBUS
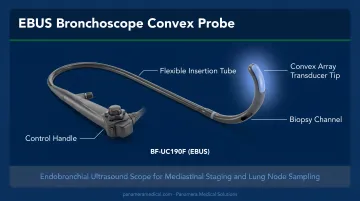
Convex Probe EBUS (CP-EBUS) and EBUS-TBNA
CP-EBUS uses a linear, curved-array transducer at 7.5 MHz mounted at the bronchoscope tip. It generates images parallel to the scope's insertion axis — the configuration that enables real-time needle aspiration.
Accessible lymph node stations via CP-EBUS:
- Paratracheal: 2R, 2L, 4R, 4L
- Subcarinal: 7
- Hilar: 10R, 10L, 11R, 11L
- Para-esophageal/posterior: 3P
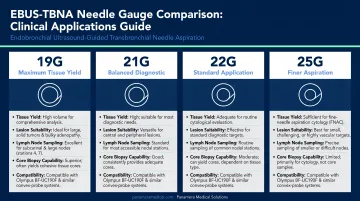
EBUS-TBNA (transbronchial needle aspiration) is performed through the CP-EBUS working channel. Available needle sizes and their typical uses:
| Gauge | Primary Application |
|---|---|
| 25G | Cytology, molecular testing in malignancy |
| 22G | Standard cytology and cell-block |
| 21G | Larger histologic material, granulomatous disease |
| 19G | Core biopsy, lymphoma workup, tissue architecture |
Where CP-EBUS excels in central airway staging, it cannot reach peripheral nodules beyond the central airways — the domain where RP-EBUS fills the gap.
Clinical Applications and Indications
NSCLC Staging and Diagnosis
EBUS-TBNA is the preferred first-step procedure when mediastinal nodal involvement is suspected in non-small cell lung cancer. A 2009 meta-analysis of 1,299 patients by Gu et al. reported a pooled sensitivity of 0.93 and specificity of 1.00 for mediastinal staging — figures that have held up in subsequent studies.
Compared to conventional TBNA, the advantage is clearest for smaller nodes. Herth et al. demonstrated sampling of nodes with a mean diameter of just 1.6 cm (range 0.8–3.2 cm), and a randomized comparison showed EBUS-TBNA diagnostic yield of 66.7% versus 33.3% for conventional TBNA.
A few technique points matter for accuracy:
- Sample in N3 → N2 → N1 order to prevent upstaging from needle contamination
- For restaging after neoadjuvant therapy, positive results remain reliable, but negative results carry a low NPV and may require surgical confirmation
Sarcoidosis
The ATS 2020 clinical practice guideline recommends EBUS-guided lymph node sampling rather than mediastinoscopy as the initial procedure when tissue is needed for suspected sarcoidosis. The randomized GRANULOMA trial demonstrated granuloma detection rates of 80% with endosonography versus 53% with conventional bronchoscopy (P < .001).
EBUS is particularly useful in early-stage sarcoidosis, where adenopathy may be present but parenchymal changes are minimal — exactly the scenario where conventional bronchoscopic biopsy tends to underperform.
Lymphoma
EBUS-TBNA is an acceptable initial minimally invasive test for suspected lymphoma per ACCP guidance, but with important caveats. Overall diagnostic sensitivity is around 65%, and negative results do not exclude disease. Hodgkin lymphoma remains a particular limitation because tissue architecture is needed for definitive subtyping.
Sensitivity is higher in recurrent lymphoma, where the clinical context narrows differential diagnosis. When lymphoma is suspected, a 19G needle is preferred to obtain larger core material that preserves tissue architecture for classification.
Tuberculosis, Infections, and Mediastinal Masses
For intrathoracic TB presenting with lymphadenopathy, a CHEST meta-analysis reported pooled EBUS-TBNA sensitivity of 0.80 and specificity of 1.00. Bacterial and fungal culture sensitivity remains a limitation when ruling out infectious etiologies.
For mediastinal masses of unknown etiology, EBUS-TBNA consistently achieves tissue diagnosis across a range of pathologies. It can also serve a limited therapeutic role — draining mediastinal cysts such as bronchogenic cysts — though recurrence rates remain high and current evidence supports this only as an adjunct, not a standalone intervention.
Molecular testing: EBUS-TBNA samples are adequate for biomarker and molecular profiling in NSCLC. A median of 4 passes yields adequate molecular profiling material in approximately 95% of cases.
How the EBUS Procedure Works
Pre-Procedure Preparation
Standard preparation includes:
- Fasting: At least 2 hours for clear liquids, 4 hours for light meals before the procedure
- Anticoagulants: Warfarin stopped at least 5 days prior (target INR <1.5); NOACs stopped at least 2 days; clopidogrel/prasugrel/ticagrelor stopped at least 5 days for higher-bleeding-risk procedures
- Platelet count: A minimum of 50,000/µL is recommended when biopsy is planned
- Contraindication screening: Unstable arrhythmias, recent MI, refractory hypoxemia, and uncorrectable severe bleeding diathesis must be assessed and addressed before proceeding
Anesthesia and Positioning
EBUS is most commonly performed under deep sedation in the United States, though moderate sedation and general anesthesia are both used. A randomized trial found no significant diagnostic yield difference between general anesthesia (70.7%) and moderate sedation (68.9%, P = 0.816); a 2018 prospective study reached the same conclusion.
Standard positioning is supine with the operator at the head of the bed. Continuous monitoring includes oxygen saturation, blood pressure, and ECG for the duration of the procedure.
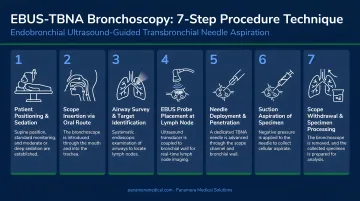
Step-by-Step Technique
- Scope insertion — via nose, mouth, LMA, or endotracheal tube (minimum size 8); tracheostomy access is also possible
- Systematic survey — identify mediastinal and hilar lymph node stations using ultrasound
- Doppler use — differentiate lymph nodes from adjacent vascular structures before any needle pass
- Balloon catheter — deploy to improve wall contact at paratracheal stations (2R, 2L, 4R, 4L) when needed
- TBNA needle technique — position scope neutrally; advance needle through working channel; stylet use is optional (evidence shows it does not improve yield); apply or withhold suction (no significant adequacy difference either way)
- Agitation — a 2022 trial found 3 agitations noninferior to 10 for malignant-cell and DNA yield
- Pass count — minimum 3 passes per node without ROSE; minimum 4 passes when molecular profiling is required
Post-Procedure Monitoring
Patients are monitored for 1–4 hours post-procedure until sedation effects resolve. Expected after-effects include mild sore throat, hoarseness, or light cough for approximately one day.
Seek immediate attention for:
- Persistent hemoptysis
- Increasing chest pain or difficulty breathing
- Fever developing within 24–48 hours
- Signs of progressive respiratory distress
Benefits Compared to Alternative Diagnostic Procedures
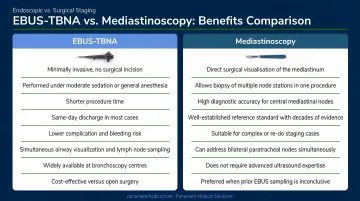
EBUS-TBNA has meaningfully displaced surgical alternatives over the past two decades. A US utilization analysis cited by Avasarala et al. found that median center mediastinoscopy rates fell from 21.6% to 10% between 2006 and 2010 — a shift directly attributable to EBUS adoption.
Why EBUS is preferred as first-line:
- No surgical incision, no general anesthesia requirement
- Outpatient-compatible with same-day discharge
- Cancer diagnosis and nodal staging achievable in a single procedure session
- Accesses lymph node stations unreachable by CT or PET guidance alone
- Lower cost and lower complication burden than mediastinoscopy
One factor that further refines EBUS procedural efficiency is Rapid On-Site Evaluation (ROSE). A CHEST meta-analysis found ROSE reduced EBUS-TBNA needle passes by a mean difference of -1.1 passes without improving overall diagnostic yield. Its primary value is operational: ROSE allows teams to confirm sample adequacy in real time, direct ancillary testing earlier, and shorten total procedural time.
Risks, Contraindications, and Safety Considerations
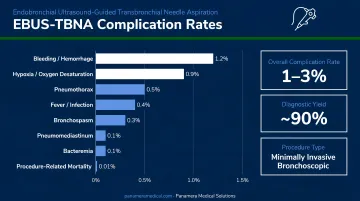
Large registries consistently report low complication rates for EBUS-TBNA:
| Complication | Rate |
|---|---|
| Total complications | 1.23–1.44% |
| Hemorrhage requiring intervention | 0.2–0.68% |
| Pneumothorax | 0.03–0.53% |
| Infectious complications | 0.19–0.48% |
| Mediastinitis | 0.10% |
| Respiratory failure | 0.07–0.23% |
Anesthesia-related risks include respiratory depression, laryngospasm, bronchospasm, and aspiration, all of which are managed through standard monitoring and staffing protocols.
Contraindications specific to EBUS-TBNA (beyond standard bronchoscopy) include:
- Active anticoagulation that cannot be bridged or held
- Coagulopathy or thrombocytopenia below safe biopsy thresholds
- Elevated creatinine/BUN affecting sedation clearance
- Elevated bleeding risk requiring individualized antithrombotic management decisions
Training and Competency
The ACCP recommends a minimum of 40–50 supervised procedures to establish basic EBUS-TBNA competency and 20 procedures annually to maintain it. Simulation-based training using validated tools like the EBUS Skills and Tasks Assessment Tool (EBUS-STAT), introduced by Davoudi et al. in 2012, is now recognized as an effective component of structured credentialing pathways.
EBUS Equipment, Technology, and Procurement Considerations
Major CP-EBUS Platforms
Three manufacturers supply the majority of CP-EBUS bronchoscopes globally:
| Manufacturer | Model | Insertion OD | Working Channel | Notable Features |
|---|---|---|---|---|
| Olympus | BF-UC190F | 6.3 mm | 2.2 mm | 20° forward oblique view, depth 2–50 mm, Doppler capable |
| Olympus | BF-UC180F | 6.9 mm | 2.2 mm | Frequencies 5/7.5/10/12 MHz, 60° scan range |
| Pentax/Hoya | EB19-J10U | ~6.3 mm | Confirm per spec | 5–10 MHz switchable, B-mode/color/pulse Doppler |
| Fujifilm | EB-530US | 6.3 mm | 2.0 mm | 120° field of view, 10° forward oblique, depth 3–100 mm |
| Fujifilm | EB-710US | 5.9 mm (insertion) | 2.2 mm | Balloon-less design, 120° FOV, 180° acute bending |
Head-to-head evidence across all three manufacturers is limited. Working channel diameter, Doppler quality, needle portfolio compatibility, ergonomics, processor compatibility, and service network often matter more in practice than minor specification differences.
Equipment Lifecycle and Upgrade Planning
Several factors drive equipment assessment cycles in EBUS programs:
- Rising institutional EBUS volume requiring higher-throughput scopes
- Evolving molecular testing demands that depend on consistent sample quality
- Generational imaging improvements, including elastography and enhanced Doppler sensitivity
Robust multi-manufacturer data linking image resolution alone to diagnostic yield improvement remains unproven, so procurement decisions typically weigh workflow fit and service network alongside specs.
Healthcare facilities evaluating EBUS equipment upgrades — or looking to replace aging bronchoscopes — can work with specialized endoscopy equipment trading partners like Panamera Medical Solutions. With over 15 years of international endoscopy trading experience across North America, Europe, and South America, Panamera Medical offers trade-in and buy-back programs for used EBUS scopes — including models from Olympus, Pentax, and Fujifilm.
This gives facilities a cost-effective way to access newer-generation devices without writing off older equipment entirely.
Frequently Asked Questions
What is the difference between bronchoscopy and EBUS?
Bronchoscopy is the broader procedure — a flexible lighted scope used to visualize the airways. EBUS is a specialized form that integrates an ultrasound transducer into the scope tip, enabling real-time imaging beyond the airway wall and simultaneous tissue sampling in a single procedure.
What conditions is EBUS used to diagnose?
Primary indications include lung cancer staging and diagnosis, sarcoidosis, lymphoma, tuberculosis and other infectious causes of lymphadenopathy, mediastinal masses of unknown etiology, and peripheral pulmonary nodules (via radial probe).
How long does an EBUS procedure take, and is it painful?
The procedure typically takes 30–90 minutes and is performed under sedation or general anesthesia, so patients feel nothing during it. Mild sore throat, hoarseness, or cough may persist for roughly a day afterward.
How does EBUS compare to mediastinoscopy for lung cancer staging?
EBUS-TBNA is minimally invasive, outpatient-feasible, and carries lower complication risk and cost than mediastinoscopy. It is now the preferred first-line staging tool. Mediastinoscopy is reserved for cases where EBUS results are negative or inconclusive but clinical suspicion remains high.
How many passes are needed during EBUS-TBNA for an adequate sample?
At least 3 passes per lymph node are recommended without ROSE. When molecular profiling is required, at least 4 passes are needed to achieve adequate sample volume in the majority of cases, based on published data from Yarmus et al.
What training is required to perform EBUS competently?
The ACCP recommends a minimum of 40–50 supervised procedures to establish competency, with at least 20 procedures annually to maintain it. Simulation-based training with validated tools like EBUS-STAT is an accepted part of structured competency programs.