Introduction
Choosing the wrong endoscope doesn't just complicate a procedure—it can cause it to fail entirely. A forward-viewing gastroscope physically cannot provide the en-face papilla view required for selective biliary cannulation. A duodenoscope is unnecessary overhead for a routine upper GI evaluation. Yet scope selection decisions get made based on availability rather than clinical indication.
For endoscopists, the distinction between these two instruments is fundamental. For procurement teams and biomedical engineers, the choice carries real financial and operational weight: acquisition costs, reprocessing complexity, and regulatory exposure all vary significantly between the two.
This guide covers what separates these two instruments — and how to act on that knowledge:
- Structural and functional differences between duodenoscopes and gastroscopes
- Clinical indications that determine which scope belongs in each procedure
- Infection control profiles and reprocessing implications
- Equipment decision-making criteria for facilities and procurement teams
Key Takeaways
- Side-viewing duodenoscopes are purpose-built for ERCP; their lateral lens and elevator mechanism make biliary cannulation possible
- Forward-viewing gastroscopes cover the full range of upper GI diagnostics and therapeutics, with no elevator mechanism for biliary access
- Contamination risk is scope-specific: the duodenoscope's forceps elevator recess has no equivalent in forward-viewing designs
- When anatomy is surgically altered — Billroth II, Roux-en-Y — forward-viewing instruments often outperform or replace duodenoscopes entirely
- Scope choice is procedure-driven and anatomy-driven—not interchangeable
Side-Viewing Duodenoscope vs Forward-Viewing Gastroscope: Quick Comparison
The table below summarizes the core differences between these two scope types — from optics and mechanics to clinical use cases and reprocessing demands.
| Feature | Side-Viewing Duodenoscope | Forward-Viewing Gastroscope |
|---|---|---|
| Lens orientation | Lateral (perpendicular to scope axis) | Forward (aligned with scope axis) |
| Elevator mechanism | Yes — Albarran lever for instrument angulation | No |
| Working channel | 4.2 mm (therapeutic) | 2.8–3.7 mm |
| Primary indication | ERCP (biliary/pancreatic access) | Upper GI endoscopy (EGD) |
| Reprocessing complexity | High — elevator recess is a contamination risk | Standard — no complex recesses |
| Altered anatomy use | Limited — cannot access papilla post-Billroth II/RYGB | Preferred — forward view aids navigation |
| Regulatory scrutiny | FDA oversight, manufacturer recalls | Standard high-level disinfection protocols |
What Is a Side-Viewing Duodenoscope?
The side-viewing duodenoscope is a specialized therapeutic endoscope built for one primary destination: the second portion of the duodenum, where the Ampulla of Vater sits. Its lateral-facing objective lens distinguishes it from every other flexible endoscope in a typical endoscopy suite.
Key Design Features
Three components define this instrument's clinical capability:
- Oblique/lateral lens provides a perpendicular view of the duodenal wall, letting the endoscopist see the major papilla face-on rather than in profile
- Forceps elevator (Albarran lever) pivots at the distal tip to deflect exiting instruments by up to nearly 90 degrees, enabling precise angulation toward the biliary or pancreatic orifice
- 4.2 mm working channel accommodates the full range of ERCP accessories: sphincterotomes, stone retrieval baskets, biliary catheters, and stents
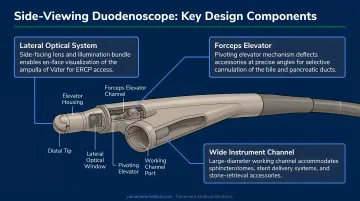
The elevator mechanism is what makes selective cannulation possible. Without it, an instrument exiting the working channel travels parallel to the scope axis—angled away from the papilla in a way that makes biliary access geometrically unreliable.
Scope Subtypes Worth Knowing
- Standard therapeutic duodenoscopes (e.g., Olympus TJF-Q190V): The workhorse for most ERCP programs
- Large-channel models: For oversized accessories or complex extractions
- Single-use/disposable duodenoscopes: Developed in response to elevator recess contamination risk; eliminate reprocessing concerns but carry considerably higher per-procedure cost
Clinical Use Cases
According to the FDA, duodenoscopes are used in more than 500,000 ERCP procedures annually in the United States. The scope's applications include:
- Bile duct stone extraction
- Biliary stenting for benign strictures or malignancy
- Pancreatic duct cannulation and stenting
- Sphincterotomy
- Tissue sampling from the ampulla
- Management of post-operative biliary complications (anastomotic strictures, leaks)
- Periampullary tumor evaluation
Across each of these indications, the side-viewing design is clinically required: no other endoscope geometry reliably achieves en-face access to the major papilla.
What Is a Forward-Viewing Gastroscope?
The forward-viewing gastroscope (more precisely, the esophagogastroduodenoscope or EGD scope) advances through the GI tract with its lens aligned to the direction of travel. The endoscopist sees exactly what lies ahead—making navigation through the esophagus, stomach, and proximal duodenum intuitive and continuous.
Key Design Features
- Forward optics: Field of view typically 140 degrees for most standard models (with a range of 90–170 degrees across the broader GI endoscope category)
- Working channel: 2.8 mm in standard diagnostic models (e.g., Olympus GIF-HQ190), 3.7–3.8 mm in therapeutic models (e.g., Olympus GIF-1TH190, Pentax EG34-i10)
- No elevator mechanism: Accessories exit parallel to the scope axis; this simplifies both manipulation and reprocessing
- Two- or four-way tip deflection: Standard for navigation
A forward-viewing scope can physically reach the second portion of the duodenum. The limitation is orientation: without a lateral lens and elevator, it cannot achieve the en-face papilla view or the precise instrument angulation that selective biliary cannulation demands.
Scope Variants Relevant to This Comparison
- Standard diagnostic gastroscopes: For routine upper GI evaluation
- Therapeutic (large-channel) gastroscopes: 3.7–3.8 mm channels for hemostasis, banding, and larger accessories
- Pediatric gastroscopes: Smaller diameter for pediatric or narrow-lumen cases
- Forward-viewing enteroscopes: Used for ERCP in surgically altered anatomy where neither a standard gastroscope nor a duodenoscope can access the papilla
Clinical Use Cases
The forward-viewing gastroscope covers the full breadth of upper GI medicine:
- Evaluation of dysphagia, reflux, and peptic ulcer disease
- Gastric cancer screening and Barrett's esophagus surveillance
- Variceal band ligation
- Hemostasis for upper GI bleeding
- Foreign body removal
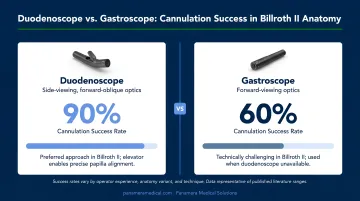
- ERCP in altered anatomy: Patients with Billroth II gastrectomy or Roux-en-Y reconstruction, where a standard duodenoscope cannot access or correctly orient to the papilla
In Billroth II anatomy, comparative data favors the forward-viewing approach. A prospective comparative trial found papilla cannulation success of 87% with a forward-viewing endoscope versus 68% with a side-viewing duodenoscope, with four jejunal perforations occurring in the side-viewing group and none in the forward-viewing group. A more recent comparison reported adverse events of 8% with duodenoscopes and 0% with gastroscopes in this population.
Roux-en-Y gastric bypass patients present a different challenge: longer limb lengths often make the papilla inaccessible to both a standard gastroscope and a duodenoscope. Device-assisted enteroscopy is the standard approach here, with balloon enteroscopy-assisted ERCP achieving total procedure success of 88.1% in one study.
Which Should You Choose?
The foundational rule is simple: scope selection is procedure-driven, not preference-driven.
The Primary Decision Framework
| Scenario | Correct Instrument |
|---|---|
| ERCP in normal anatomy | Side-viewing duodenoscope |
| Upper GI evaluation (EGD) | Forward-viewing gastroscope |
| Barrett's surveillance, variceal banding | Forward-viewing gastroscope |
| ERCP in Billroth II anatomy | Forward-viewing gastroscope or enteroscope |
| ERCP in Roux-en-Y gastric bypass | Device-assisted enteroscope (forward-viewing) |
| Hepaticojejunostomy access | Enteroscope (forward-viewing) |
These instruments are not interchangeable. A gastroscope cannot replace a duodenoscope for standard ERCP, and using a duodenoscope in Billroth II anatomy creates genuine patient safety risk.
Reprocessing: A Practical Difference
The duodenoscope's elevator recess contains small crevices that are difficult to decontaminate — and the consequences are well documented. Between 2012 and spring 2015, closed-channel duodenoscopes were linked to at least 25 outbreaks or infection incidents affecting at least 250 patients worldwide, predominantly involving carbapenem-resistant Enterobacteriaceae (CRE).
FDA postmarket surveillance found that up to 3% of properly reprocessed duodenoscopes still tested positive for organisms likely to cause infection. Older models showed 4–6% high-concern organism contamination; newer designs reduced this to around 1.1%, but the risk was never eliminated entirely.
Forward-viewing gastroscopes carry none of this burden. No elevator recess, no complex crevices, standard high-level disinfection protocols.
Those reprocessing realities translate directly into procurement decisions.
Facility-Level Considerations
For procurement teams and department managers:
- High ERCP volume programs require a therapeutic duodenoscope — reusable per-procedure reprocessing runs approximately $232 at 200 ERCPs/year (excluding infection-related costs)
- Low ERCP volume facilities should weigh total cost of ownership carefully — a new Olympus TJF-Q190V lists at approximately $63,500, before reprocessing infrastructure
- Single-use duodenoscopes run $797–$2,068 per procedure versus $612–$1,362 for reusable models; they make financial sense for high-risk patients or facilities without robust reprocessing capability
- Gastroscopes offer broader procedure coverage, lower acquisition cost, and simpler reprocessing across most GI programs

The practical recommendation for a fully equipped endoscopy unit: maintain both. They serve different clinical purposes and are complementary instruments.
Equipment Lifecycle, Costs, and Acquisition
Sticker price tells only part of the story. Total cost of ownership for duodenoscopes and gastroscopes diverges significantly once reprocessing, repair cycles, and regulatory exposure are factored in.
What Drives Cost Differences
- Duodenoscopes require more intensive reprocessing validation, periodic microbiological surveillance culturing, and potential single-use component upgrades
- Reprocessing failures carry regulatory and liability exposure that gastroscopes do not
- Repair costs and turnaround times for high-use therapeutic duodenoscopes can disrupt ERCP program continuity
Key questions for procurement teams when sourcing either scope type:
- Is the scope compatible with your existing processor system (Olympus EVIS, Pentax EPK, Fujifilm VP series)?
- What warranty coverage is provided, and what does it exclude?
- What are the repair turnaround times, and is a loaner scope available during downtime?
- Does the supplier provide documented, verified reprocessing and service history?
The Role of the Secondary Market
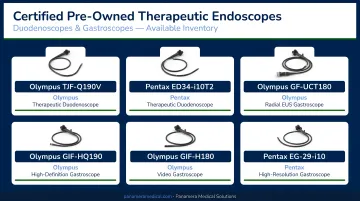
Many facilities are managing these costs by sourcing certified pre-owned or refurbished equipment. A well-sourced refurbished duodenoscope or gastroscope can deliver the same procedural capability at a fraction of new acquisition cost, provided the supplier has verified scope function, optical quality, channel integrity, and service history.
Panamera Medical Solutions sources and trades pre-owned therapeutic duodenoscopes including the Olympus TJF-Q190V and Pentax ED34-i10T2, along with gastroscopes including the Olympus GIF-HQ190, GIF-H180, and Fujifilm EG-760R. Trade-In and Buy-Back programs let facilities recoup value from aging or underused equipment, either as credit toward upgraded models or as a direct buyout.
With over 15 years of international trading experience across North America, Europe, and South America, Panamera connects facilities with a global buyer and seller network that reduces sourcing lead times for urgent replacements.
For facilities evaluating their current endoscopy inventory—whether adding a therapeutic duodenoscope, replacing an aging gastroscope, or looking to trade in equipment that no longer fits their service line—contact Panamera Medical Solutions for an equipment consultation.
Frequently Asked Questions
Is a side-viewing duodenoscope the same as an ERCP scope?
Yes — "ERCP scope" is the colloquial term; duodenoscope is the formal name for the same instrument. It features a lateral-facing lens designed for duodenal access and ampullary procedures. Side-viewing endoscopy is not synonymous with ERCP itself, but the duodenoscope is the standard instrument used to perform it.
Can a forward-viewing gastroscope be used for ERCP?
In patients with surgically altered anatomy—Billroth II gastrectomy or Roux-en-Y reconstruction—a forward-viewing scope or enteroscope is often the correct choice because a standard duodenoscope cannot reach or orient to the papilla. In patients with normal anatomy, it is not a routine substitute; selective cannulation success rates are lower and technical difficulty is higher.
Why do duodenoscopes have a higher infection risk than gastroscopes?
The forceps elevator recess at the duodenoscope tip contains small crevices that standard high-level disinfection may not fully decontaminate. This has made it a reservoir for multidrug-resistant organisms including CRE, prompting FDA safety communications, manufacturer design changes, and the development of single-use models. Forward-viewing gastroscopes have no equivalent structural vulnerability.
What is the working channel difference, and why does it matter?
Therapeutic duodenoscopes have a 4.2 mm working channel versus 2.8–3.7 mm in gastroscopes. The larger channel accommodates ERCP-specific accessories—sphincterotomes, stone retrieval baskets, and large biliary stents—that simply will not pass through a standard gastroscope channel.
Are single-use duodenoscopes worth the cost?
Single-use duodenoscopes eliminate reprocessing-related infection risk but carry per-procedure costs of $797–$2,068 versus $612–$1,362 for reusable models (cost varies by volume and assumed infection rates). They make the most sense for high-risk patients, outbreak scenarios, or facilities without robust reprocessing infrastructure. High-volume ERCP programs with strict reprocessing protocols generally favor reusable instruments for cost efficiency.
How do I know when it's time to replace or upgrade a scope?
Watch for these signals:
- Degraded image quality or recurring repair needs
- Incompatibility with updated processor systems
- Reprocessing audit failures
- New clinical service lines requiring different instrument capabilities
Compare your equipment's age against manufacturer lifecycle recommendations to determine whether repair, trade-in, or replacement makes the most financial sense.