Introduction
Standard adult colonoscopes work well — until they don't. Patients with tortuous sigmoid anatomy, prior pelvic surgery, or post-radiation adhesions regularly push standard equipment past its limits, resulting in incomplete procedures, missed diagnoses, and the considerable burden of rescheduling.
Pediatric colonoscopes belong in two distinct roles: as the appropriate primary instrument in pediatric GI endoscopy, and as a dependable rescue or preferred option in select adult cases where standard scopes fall short. Clinical evidence supports both applications.
What follows is a practical breakdown of those clinical applications, the measurable advantages pediatric colonoscopes deliver, and the operational costs of not having the right instrument available.
Key Takeaways
- Pediatric colonoscopes (typically 10–12 mm OD) offer smaller diameter and greater shaft flexibility than standard adult scopes
- Validated for both pediatric GI endoscopy and as a rescue tool in anatomically difficult adult cases
- Cecal intubation rates are comparable to adult scopes in routine colonoscopy — 91% vs. 93% in one RCT
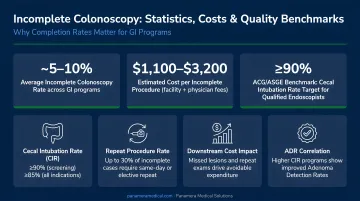
- Incomplete colonoscopy rates reach 4%–25% — the pediatric scope directly addresses this failure point in complex cases
- Stocking a pediatric colonoscope alongside adult scopes — including refurbished models — expands case completion without adding new-equipment costs
What Is a Pediatric Colonoscope?
A pediatric colonoscope is a slimmer, more flexible variant of the standard colonoscope. Pediatric and slim colonoscopes cluster around a 10–12 mm outer diameter: the Olympus PCF-H190L measures 11.7 mm, while an adult scope like the Olympus CF-HQ190L sits at 13.2 mm. Working channels typically run 2.8–3.8 mm, retaining full functionality for biopsy and therapeutic tools.
The name implies exclusive pediatric use, but that's not how endoscopists actually deploy these instruments. Pediatric colonoscopes appear routinely in adult endoscopy suites as either a secondary rescue scope or the preferred first-choice instrument for specific patient presentations, including:
- Fixed or angulated sigmoid colons
- Post-surgical anatomy
- Luminal strictures
A pediatric colonoscope is a specialized instrument that expands what an endoscopy unit can accomplish when standard equipment reaches its limits. In certain patient populations, it performs just as well as the adult scope from the outset.
Key Clinical Applications and Advantages
The value of pediatric colonoscopes is best understood through their real-world clinical impact: higher procedural completion rates, fewer repeat scopes, and better outcomes in specific populations. Three distinct advantages account for most of that value.
Advantage 1: Superior Maneuverability Through Complex Anatomy
The smaller diameter and increased shaft flexibility of pediatric colonoscopes allow them to navigate anatomical challenges that routinely halt standard adult scopes, including fixed or angulated sigmoid colons and post-surgical adhesions.
The clinical picture is clear: when an adult scope cannot advance through a tight or angulated sigmoid segment, switching to a pediatric colonoscope often completes the procedure without abandonment or rescheduling. Marshall et al. (1996) found the pediatric scope successfully reached the cecum in over 58% of cases where the adult scope had already failed, a meaningful rescue rate for what would otherwise be incomplete examinations.
Why this matters operationally:
- Incomplete colonoscopy rates range from 4% to 25% across published reports, with tortuous colon accounting for roughly 30% of failures
- Incomplete examinations are associated with higher rates of interval proximal colon cancer — one review estimates the risk approximately doubles
- Average colonoscopy episode costs were reported at $2,146 (commercial) and $1,071 (Medicare) in claims data; each avoidable repeat procedure adds direct cost beyond clinical risk
- The ASGE/ACG 2024 quality indicators now set a ≥95% cecal intubation rate as the performance benchmark, raising the bar for completion
Patient subgroups where this advantage is most clinically relevant:
- Women with prior hysterectomy, pelvic surgery, radiation therapy, or endometriosis
- Patients with a history of sigmoid diverticulitis
- Those with known or suspected colonic strictures
- Low-BMI patients, who show significantly higher incomplete colonoscopy risk
The pediatric colonoscope functions as a reliable rescue instrument that directly addresses the most common failure point in difficult-anatomy cases.
Advantage 2: Broader Clinical Applicability Across Patient Populations
The primary application is in children requiring colonoscopy for rectal bleeding, chronic abdominal pain, persistent diarrhea, polyp removal, or suspected IBD, where smaller anatomy requires a proportionally sized instrument. Published multicenter data places lower GI bleeding (27.1%), abdominal pain or bloating (20.3%), diarrhea (14.2%), and IBD (8.5%) as the leading indications.
The same scope also serves as a legitimate alternative in adult endoscopy. Saifuddin et al. (2000) randomized 150 adults and found cecal intubation rates of 93% with the pediatric colonoscope versus 91% with the adult scope, establishing the pediatric instrument as suitable for routine adult colonoscopy, not just rescue use. A 2022 study by Alkhatib et al. found pediatric colonoscope use was associated with higher terminal ileum intubation rates (72.1% vs. 58.8%) compared to adult scopes.
This dual-use value has practical procurement implications:
- A single instrument category serves two distinct patient populations and multiple clinical indications
- Facilities managing both pediatric referrals and complex adult cases don't need separate specialized equipment for each scenario
- Endoscopy units with both scope types can accept a broader referral base without expanding their equipment footprint
Best suited for: Hospitals or ambulatory endoscopy centers managing mixed pediatric and adult GI services; facilities receiving referrals for difficult adult cases; centers looking to expand procedural capabilities without significant capital outlay.
Advantage 3: Procedural Efficiency in Select Cases
When the pediatric colonoscope is the right instrument for the case, its use can reduce procedure time, minimize looping in the colon, and decrease the physical discomfort associated with scope advancement. Reduced shaft stiffness limits the paradoxical motion and loop formation common in tortuous colons, allowing more direct advancement with less force.
In adult patients, this may reduce sedation requirements. In pediatric patients (where colonoscopy is performed under deep sedation or with anesthesia support), scope handling precision directly affects procedure duration — minimizing anesthetic exposure time is a clinical priority, and every reduction in manipulation time contributes to that goal.
NASPGHAN's pediatric GI endoscopy unit guidelines cite a scheduling model that allocates 60 minutes for pediatric colonoscopy including anesthesia induction, procedure, recovery, and turnover, with anesthesiologist-administered sedation adding 10–15 minutes. Any reduction in scope manipulation time contributes directly to that window.
Operational metrics affected by this advantage:
- Mean procedure time
- Sedation dosage per case
- Patient-reported comfort scores
- Recovery room time
- Procedure throughput per session
What Happens When the Right Scope Isn't Available
When an endoscopy unit relies solely on standard adult colonoscopes, a predictable set of clinical and operational problems follows:
- Incomplete procedures accumulate. Failed examinations in anatomically complex patients lead to missed diagnoses and repeat scheduling — carrying the same preparation burden and cost as the original visit
- Pediatric referrals get turned away. Without appropriate instrumentation, facilities cannot accommodate pediatric patients, limiting their service range and sending referrals elsewhere
- Endoscopists face unnecessary procedural risk. Managing difficult adult cases without a flexible alternative increases looping force, mucosal trauma, and patient discomfort, all of which affect complication rates and patient experience scores
- Costs accumulate. Repeat colonoscopy within four years occurs at rates of 12.6% (commercial) and 19.8% (Medicare) based on claims data, and while not all repeats are avoidable, those driven by equipment limitations represent preventable cost
Each of these problems has a straightforward solution: access to the right scope for the right case.
How to Get the Most Value from Pediatric Colonoscopes
Owning the instrument is just the starting point — full value comes from building deliberate operational habits around it:
- Establish clear case-selection protocols. Decide upfront when the pediatric colonoscope is the first-line choice versus a rescue instrument in adult cases. Without defined criteria, the scope stays on the shelf.
- Track outcomes by scope type. Reviewing cecal intubation rates, procedure time, sedation doses, and patient comfort scores at the scope level helps refine case selection and surfaces the patient subgroups where the pediatric instrument consistently outperforms.
- Calculate the fully loaded cost of incomplete procedures. Repeat bookings, sedation, staff time, and patient preparation add up quickly. Once those costs are on paper, the case for maintaining both scope types becomes clear.
- Offset acquisition costs through trade-in programs. Facilities adding the Olympus PCF-H190L or PCF-H190DL can apply older adult colonoscopes (such as the CF-H180) toward the purchase through Panamera Medical Solutions' trade-in and buy-back program, reducing net cost without absorbing full new-unit pricing.
Conclusion
The clinical value of pediatric colonoscopes comes down to one thing: extending procedural reach. They enable successful colonoscopy in patients where standard instruments fail, serve pediatric populations appropriately, and improve efficiency in cases where anatomy demands a more flexible approach.
Maintaining access to both instrument types compounds that value across your endoscopy program. Cases that would otherwise be abandoned become completed diagnostic procedures — meaning fewer repeat bookings, cleaner diagnostic records, and less strain on scheduling.
For facilities evaluating their colonoscope inventory, the question isn't whether pediatric scopes add value — it's whether your current setup leaves that value on the table.
Frequently Asked Questions
Why use a pediatric colonoscope on an adult?
Adults with anatomically challenging colons (fixed or angulated sigmoid segments, prior pelvic surgery, or strictures) benefit from the pediatric scope's smaller diameter and greater flexibility. Where a standard adult scope cannot advance, the pediatric instrument allows the procedure to be completed rather than abandoned.
What is the diameter of a pediatric colonoscope?
Pediatric and slim colonoscopes typically have outer diameters in the range of 10–12 mm — the Olympus PCF-H190L, for example, measures 11.7 mm. Exact dimensions vary by manufacturer and model generation, so confirm specifications for the specific instrument in use.
Can a 4-year-old get a colonoscopy?
Yes. Colonoscopy is performed in young children when clinically indicated, using appropriately sized pediatric instrumentation and deep sedation or anesthesia support. Age, weight, and clinical indication together guide scope selection and bowel preparation protocols.
How does a pediatric colonoscope differ from a standard adult colonoscope?
The key differences are a smaller outer diameter, greater shaft flexibility, and a narrower working channel that still accommodates biopsy forceps and standard therapeutic tools. Core imaging, air/water, and suction functions remain the same as on the adult instrument.
What conditions are diagnosed with colonoscopy in children?
Primary indications include rectal bleeding, chronic abdominal pain, persistent diarrhea, suspected inflammatory bowel disease, and polyp detection or removal. Unexplained iron-deficiency anemia and weight loss are also recognized indications in the pediatric population.
What are the risks of colonoscopy in pediatric patients?
Pediatric colonoscopy is generally safe when performed by experienced pediatric gastroenterologists, with multicenter data reporting an immediate complication rate of approximately 1.1%. Risks include bleeding (the most common event, particularly after polypectomy), perforation, and sedation-related effects, all of which are discussed with families during informed consent.