The decision between single-use and reusable bronchoscopes has never been straightforward, but it's become harder to defer. Infection control standards have tightened, reprocessing bottlenecks are disrupting scheduling in busy units, and cost pressures are forcing procurement teams to scrutinize total cost of ownership rather than just purchase price.
This guide walks through what the published evidence actually shows — on cost, turnaround time, infection risk, and environmental impact — so your facility can make a deliberate, data-grounded choice.
Key Takeaways
- Single-use bronchoscopes eliminate cross-contamination risk and require zero reprocessing time, but carry a fixed per-procedure cost and generate more medical waste.
- Reusable bronchoscopes amortize well at high volumes, but reprocessing runs ~49 minutes per scope — up to ~83 minutes with drying and delays.
- Reusable bronchoscopy costs $266–$406 per procedure; single-use runs $249–$403 — comparable ranges with different cost drivers.
- No universal winner exists: procedure volume, patient population, infrastructure, and budget model all determine which approach makes more sense.
- A hybrid inventory — reusable for scheduled procedures, single-use for emergencies and isolation cases — is an increasingly common middle-ground strategy.
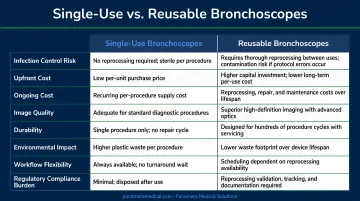
Single-Use vs. Reusable Bronchoscopes: Quick Comparison
| Dimension | Single-Use | Reusable |
|---|---|---|
| Initial Cost | Low — no capital equipment investment | High — scope purchase plus reprocessing infrastructure |
| Per-Procedure Cost | Fixed and predictable ($249–$403) | Variable; $266–$406 depending on volume, repairs, reprocessing |
| Reprocessing Time | Zero | ~49 min active; up to ~83 min total |
| Infection Risk | Negligible cross-contamination | Protocol-dependent; documented outbreaks on record |
| Image Quality | Comparable for routine procedures; premium reusables still lead for complex interventions | Superior for advanced interventional procedures |
| Maintenance Burden | None | Repair costs, AER maintenance, staff training |
| Environmental Impact | Higher per-procedure plastic waste | Lower waste per use, but higher water, chemical, and energy consumption |
| Ideal Clinical Setting | Emergency, ICU, isolation, low-volume, remote | High-volume bronchoscopy suites, interventional programs |
What Are Single-Use Bronchoscopes?
Single-use (disposable) bronchoscopes are factory-sterilized, pre-packaged flexible scopes designed for a single patient encounter and then discarded. Each scope arrives sterile at the point of use — reprocessing isn't required, AER availability isn't a factor, and there's no turnaround wait between consecutive patients.
This operational simplicity matters most in settings where contamination risk is high or reprocessing infrastructure is unavailable: ICUs, isolation rooms, bedside procedures, emergency departments, and remote clinical environments.
Technology and Image Quality
Early disposable scopes drew criticism for inferior optics. That gap has narrowed. A prospective controlled study of 45 patients (He et al., BMC Pulmonary Medicine, 2023) found comparable image clarity and biopsy positivity rates (100% in both groups), with mean routine exam times of 3.40 minutes for single-use vs. 3.55 minutes for reusable. Ultra-high-end imaging for complex interventional procedures still favors premium reusable models, but for the majority of diagnostic bronchoscopies, single-use scopes perform comparably.
Limitations Worth Noting
- Per-procedure cost is fixed and doesn't improve with volume — at scale, this adds up
- Depends on an uninterrupted supply chain for consistent availability
- Generates more per-procedure plastic and medical waste than reusable alternatives
Use Cases for Single-Use Bronchoscopes
Single-use scopes are the preferred or practical choice in:
- Emergency and trauma units where immediate scope availability is non-negotiable
- Isolation rooms housing immunocompromised or infectious patients
- ICU settings where bedside procedures are common and transport to reprocessing is impractical
- Low-volume bronchoscopy centers where reprocessing infrastructure costs outweigh benefits
- Remote or field settings without access to AERs or trained reprocessing staff
The infection outcomes data reinforces this case. A retrospective analysis of 14,228 bronchoscopy procedures (Garrett, CHEST, 2021) found 30-day readmission rates of 3.6% for single-use versus 7.7% for reusable bronchoscopes: a meaningful difference in infection-sensitive populations.
What Are Reusable Bronchoscopes?
Reusable flexible bronchoscopes — fiberoptic or video-chip designs engineered for hundreds to thousands of uses — have been the standard of care in formal bronchoscopy suites since Shigeto Ikeda introduced the flexible fiberoptic bronchoscope in 1967. Their staying power in clinical practice reflects real advantages: premium imaging quality, well-established workflows, and strong cost efficiency at high procedure volumes.
Reprocessing Requirements
After every procedure, reusable scopes must complete a multi-step cleaning and disinfection cycle before they're safe for the next patient. Per the CDC's disinfection guidelines, bronchoscopes require high-level disinfection (HLD) at minimum.
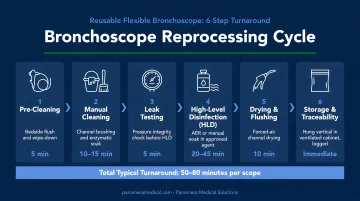
The full reprocessing sequence includes:
- Pre-cleaning at the point of use
- Leak testing
- Manual cleaning (~10 minutes)
- Transport to HLD/AER
- Automated endoscope reprocessor (AER) cycle
- Forced-air drying (~10 minutes)
A multicenter prospective study (Islam et al., CHEST, 2024) measured active setup and reprocessing time at ~49 minutes, with total time reaching ~83 minutes when delays and forced-air drying are included. The average observed bronchoscopy procedure duration in the same study was ~46 minutes — meaning reprocessing can exceed the procedure itself.
That reprocessing burden connects directly to the limitations facilities encounter in practice.
Limitations
- Reprocessing bottlenecks create scheduling gaps when scope turnover exceeds availability
- Repair and maintenance costs are variable and can be difficult to forecast
- Microbial contamination risk rises when reprocessing protocols lapse — one study reported a cross-contamination rate of 8.7% across 1,664 samples (Travis et al., 2023)
- Significant capital investment required for both scopes and reprocessing infrastructure
Use Cases for Reusable Bronchoscopes
Reusable scopes are the better fit when:
- Procedure volume is high — the cost-efficiency case improves above breakeven thresholds
- Advanced interventional bronchoscopy is performed, where superior optics and instrument channel performance matter
- Dedicated reprocessing staff and AER infrastructure are in place and functioning reliably
- Established bronchoscopy programs already have familiar clinical workflows and trained personnel
On breakeven volume: a 2022 meta-analysis (Andersen et al., PharmacoEconomics Open) estimates the crossover point at 306 procedures per site per year, or 39 procedures per scope annually. In a US high-volume academic setting, a separate 2023 model placed the breakeven at 756 procedures per site per year.
Which Is Right for Your Facility?
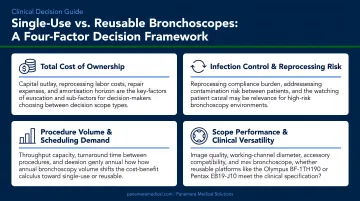
Four factors drive this decision. Evaluate each honestly before settling on a strategy.
The Four Primary Decision Factors
- Annual procedure volume — The cost efficiency of reusable scopes depends entirely on volume. Below ~306 procedures per year, single-use is often more economical when full reprocessing infrastructure costs are factored in.
- Infection control priorities — If your patient population includes immunocompromised individuals, transplant recipients, or patients with active infections, the infection risk differential is clinically relevant.
- Reprocessing infrastructure and staff capacity — AERs, trained technicians, and protocol compliance aren't free. Facilities without this infrastructure in place face a steeper total cost of ownership for reusable scopes than the per-unit price suggests.
- Budget model — Capital expenditure (reusable) vs. operational expenditure (single-use per procedure) affects how costs appear on the books, which matters for budget approval processes.
When to Choose Single-Use
- Procedure volume is low or unpredictable
- Patient population is immunocompromised or infectious
- Reprocessing staff or AER equipment are unavailable or unreliable
- Clinical setting demands immediate scope availability (emergency, ICU, bedside)
- Supply chain for reprocessing chemicals or AER maintenance parts is uncertain
When to Choose Reusable
- High annual procedure volume justifies capital investment
- Dedicated reprocessing unit and trained staff are in place
- Advanced imaging or specialized instrumentation is required
- Long-established bronchoscopy program with mature protocols
The Hybrid Model
Many high-volume facilities use a hybrid model: reusable scopes for scheduled, complex procedures, and single-use scopes for emergencies, isolation cases, and overflow when reusable units are tied up in reprocessing. This approach captures the cost efficiency of reusable equipment where volume supports it, while removing infection risk and availability constraints for unpredictable cases.
Whichever direction a facility takes, transitioning often means dealing with existing inventory. Trade-in and buy-back programs — like those Panamera Medical Solutions runs across North America, Europe, and South America — let facilities recover value from older equipment and apply it toward the transition. Older Olympus, Pentax, Fujifilm, and Karl Storz bronchoscopes typically have motivated buyers in that global network, even when local resale options are limited.
Real-World Scenarios: How Facilities Navigate the Choice
Consider a busy academic pulmonology suite running two scopes through a shared reprocessing unit. At ~46 minutes per procedure and ~83 minutes total per reprocessing cycle, a single scope effectively supports fewer than five procedures per standard shift before the bottleneck appears — not in the bronchoscopy suite, but in the AER queue.
When procedure volume grows or staffing gaps emerge in the reprocessing unit, that constraint becomes a scheduling problem — cases get delayed, rescheduled, or bumped entirely. The scope itself isn't the problem; the infrastructure behind it is.
Facilities that have recognized this pattern typically evaluate it through one of three entry points:
- An infection control audit that flags reprocessing protocol deviations
- A scheduling analysis that surfaces avoidable case delays
- A repair cost review showing annual maintenance expense has climbed past the cost of equivalent single-use coverage
The operational response depends on where the pressure is greatest. Common approaches include:
- Adding scope inventory to reduce per-scope reprocessing pressure
- Introducing single-use scopes for targeted indications — ICU patients, isolation cases, after-hours emergencies — without dismantling reusable infrastructure entirely
No procurement decision should be made from the scope catalog alone. Total cost of ownership analysis, infection risk assessment, and scheduling capacity modeling all need to feed the conversation.
Facilities re-evaluating their bronchoscope setup — whether upgrading reusable scopes or moving toward a hybrid model — can work with Panamera Medical Solutions to understand what their existing inventory is worth and what transition paths are available.
Conclusion
Single-use bronchoscopes offer safety, scheduling flexibility, and zero reprocessing overhead. Reusable bronchoscopes offer imaging excellence, procedural versatility, and long-term cost efficiency when procedure volumes support the infrastructure.
Neither approach is universally superior. The right choice depends on procedure volume, patient population, reprocessing infrastructure, and budget structure. Facilities that navigate this well typically start by auditing their current utilization data, then stress-test both models against realistic cost projections before committing.
For facilities leaning toward reusable bronchoscopes, refurbished units from established brands like Olympus or Pentax can significantly reduce the upfront capital burden — making a deliberate hybrid strategy financially viable even at mid-range volumes. Panamera Medical Solutions works with healthcare facilities across North America and beyond to source, evaluate, and trade in endoscopic equipment, including bronchoscopes, as part of a structured upgrade or cost-reduction plan.
Frequently Asked Questions
Are bronchoscopes reusable?
Traditional flexible bronchoscopes are designed for repeated use following high-level disinfection after each procedure. Single-use (disposable) bronchoscopes are also widely available — used once and discarded — and are increasingly common in infection-sensitive and low-volume clinical settings.
What are the two types of bronchoscopes?
The two primary types are rigid bronchoscopes, used under general anesthesia for specific interventional procedures, and flexible bronchoscopes. Flexible scopes are the most commonly used type, available in both reusable and single-use formats for diagnostic and therapeutic airway procedures.
How green is my reusable bronchoscope?
Research by Massart et al. (2024) found reusable scopes carry lower greenhouse-gas emissions when used more than 50 times per year. Below that threshold, reprocessing cycles — which consume chemical disinfectants, energy, and water — can offset the advantage over disposables.
How do hospitals remove mucus from lungs?
Bronchoscopy — using either a reusable or single-use flexible bronchoscope — is the primary technique for airway suctioning and mucus clearance, particularly in ICU and post-surgical patients. Chest physiotherapy and mechanical suction catheters are used alongside or instead, depending on clinical presentation.
What is the average cost per bronchoscopy procedure with a reusable scope?
Published figures vary by setting. A targeted review (Travis and Russell, Value in Health, 2020) reports $368 on average across six countries ($123 capital, $107 repair/maintenance, $139 reprocessing). A 2022 meta-analysis places the mean at $266; a 2023 US high-volume model reports $274. Estimates range with procedure volume, repair rates, and reprocessing method.
When should a hospital choose single-use over reusable bronchoscopes?
Single-use scopes are the stronger choice in several scenarios:
- Emergency or urgent-access settings where reprocessing turnaround is impractical
- Procedures on immunocompromised or infectious patients
- Facilities with limited or unreliable reprocessing capacity
- Low-volume programs where reprocessing infrastructure costs outweigh equipment reuse savings