Key Takeaways
- Fiberoptic colonoscopes use bundled glass fibers to transmit real-time images, enabling full colon visualization from anus to cecum
- Diagnostic indications include CRC screening, rectal bleeding, IBD evaluation, and post-polypectomy surveillance
- Loop management and bowel preparation quality are the two most controllable factors affecting procedure success
- Video colonoscopes offer superior image resolution, but fiberoptic scopes remain clinically functional with proper maintenance
- Facilities upgrading aging fiberoptic inventory can recover equipment value through buy-back and trade-in programs
Introduction
When Dr. William Wolff and Dr. Hiromi Shinya performed the first modern colonoscopies at Beth Israel Medical Center in June 1969, they changed the trajectory of gastrointestinal medicine. Their early series exceeded 1,600 diagnostic procedures within three years — and fiberoptic technology formed the backbone of every one of them.
Decades later, fiberoptic colonoscopes still operate in endoscopy units across the globe. Understanding the technology, procedural technique, and equipment lifecycle remains essential knowledge for clinicians, endoscopy managers, and procurement teams.
This guide covers:
- How fiberoptic colonoscopes work
- Clinical applications and procedural best practices
- Comparison with video endoscopy systems
- Reprocessing standards and equipment lifecycle management
What Is a Fiberoptic Colonoscope? History and Defining Features
A fiberoptic colonoscope is a flexible endoscope that uses bundled glass fibers to transmit light and images, allowing direct visualization of the entire large intestine — from the anus to the cecum — and, when indicated, the terminal ileum.
From Rigid Instruments to Full Colon Access
The technology traces back to Basil Hirschowitz and Larry Curtiss at the University of Michigan, whose preliminary report on the flexible fiberoptic endoscope appeared in 1957. That prototype enabled flexible passage through the upper GI tract, but colonoscopy required further development.
Dr. Niwa and Dr. Yamagata at Tokyo University extended the fiberoptic principle to lower GI endoscopy, creating the basis for full colon visualization. Wolff and Shinya brought it to clinical practice in 1969. By 1973, their landmark polypectomy paper in the New England Journal of Medicine demonstrated that polyps beyond the reach of the sigmoidoscope could be removed without surgery.
What Sets It Apart
The fiberoptic colonoscope differs fundamentally from its predecessors:
- Rigid sigmoidoscopes covered only the distal 25 cm, leaving the majority of the large bowel unseen
- Semi-flexible instruments improved on rigidity but still couldn't reliably navigate the full colon
- Fiberoptic colonoscopes use controlled four-way tip deflection to achieve total colonoscopy — and terminal ileoscopy — in an outpatient setting
Key Components and How Fiberoptic Technology Works
The Coherent Fiber Bundle
The defining component of a fiberoptic colonoscope is the coherent image bundle — thousands of individual glass fibers arranged in identical order at both ends of the bundle. Because each fiber occupies the same position at the proximal and distal ends, the image captured at the tip transmits faithfully to the eyepiece.
Each fiber is coated with cladding — a glass layer with a lower refractive index — that traps light inside the core through internal reflection. When a fiber breaks, it transmits no light, appearing as a fixed black dot in the image. Over time, accumulating fiber breakage progressively degrades image clarity.
Illumination and the Light Source
A separate, incoherent fiber bundle carries high-intensity light from an external source to the distal tip, illuminating the colon wall. Unlike the image bundle, this illumination bundle doesn't need fiber-to-fiber spatial alignment — it only needs to deliver light. The external light source unit (xenon lamp in most legacy systems) is a critical ancillary component; a failing light source directly impairs visualization regardless of fiber bundle integrity.
The Working Channel
Running alongside the fiber bundles is a hollow instrument channel — typically 3.2 to 3.8 mm in diameter on adult colonoscopes. This channel enables:
- Biopsy forceps for tissue sampling
- Polypectomy snares for polyp removal
- Electrosurgical tools for hemostasis
- Water and air insufflation
This single channel turns the colonoscope from a purely diagnostic tool into one capable of sampling, treating, and controlling bleeding in the same session.
Four-Way Tip Deflection
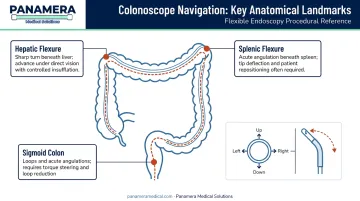
Angulation wires connect proximal control dials to the distal bending section, allowing the operator to deflect the tip up, down, left, and right. This four-way articulation is essential for navigating the colon's sharpest turns:
- Sigmoid colon loops and acute angulations
- The splenic flexure
- The hepatic flexure
Controlled tip deflection lets the endoscopist advance the scope through each curve without forcing the insertion tube against the bowel wall.
Fiberoptic vs. Video Image Capture
In fiberoptic colonoscopes, the image travels optically through glass fibers to an eyepiece or an externally attached camera head. Video colonoscopes embed a CCD or CMOS digital chip directly at the distal tip, capturing images electronically and sending them to a monitor. The clinical and operational implications of this distinction are covered in the comparison section below.
Clinical Applications: Diagnostic and Therapeutic Uses
Diagnostic Indications
Colonoscopy is the primary tool for detecting and evaluating colorectal pathology. Standard diagnostic indications include:
- CRC screening and surveillance — The USPSTF recommends screening beginning at age 45, with colonoscopy every 10 years as one accepted strategy for average-risk adults
- Rectal bleeding — both frank and occult, including iron-deficiency anemia workup
- Inflammatory bowel disease — initial diagnosis of Crohn's disease and ulcerative colitis, and monitoring of disease activity and extent
- Altered bowel habits — unexplained diarrhea or change in stool caliber
The American Cancer Society projects approximately 108,860 new colon cancer cases and 49,990 new rectal cancer cases in the United States in 2026, with about 55,230 colorectal cancer deaths — making colonoscopy one of the most consequential tools in preventive medicine.
Surveillance Colonoscopy
Post-polypectomy surveillance intervals follow USMSTF 2020 guidance:
| Finding | Recommended Interval |
|---|---|
| 1-2 tubular adenomas <10 mm | 7-10 years |
| 3-4 tubular adenomas <10 mm | 3-5 years |
| 5-10 tubular adenomas or any adenoma ≥10 mm | 3 years |
These intervals apply to average-risk polyp findings. Hereditary syndromes require more aggressive schedules:
- Lynch syndrome — colonoscopy every 1–2 years beginning at age 20–25; annual surveillance for confirmed mutation carriers (ACG guidelines)
- Classic FAP — annual surveillance beginning at puberty
Therapeutic Applications
The working channel transforms the colonoscope from a diagnostic camera into an interventional platform:
- Polypectomy using electrosurgical snare — the landmark application documented by Wolff and Shinya in their 1973 NEJM paper
- Biopsy (hot and cold) for histologic diagnosis
- Hemostasis via electrocoagulation or hemoclip placement over bleeding vessels
- Injection therapy for submucosal lesions or active hemorrhage
Terminal Ileoscopy and Alternatives
Intubation of the terminal ileum is clinically warranted when Crohn's disease is suspected or when ileocecal valve assessment is needed. Skilled operators achieve this without fluoroscopy in outpatient settings. In routine screening populations, clinical yield is lower — one 2022 study reported 40.8% overall ileal intubation with only 1.8% clinically significant histology.
When full colonoscopy is contraindicated or incomplete, ESGE guidelines identify two alternatives:
- CT colonography — preferred primary option, ideally same or next day following an incomplete procedure
- Colon capsule endoscopy — secondary option when CT colonography is not feasible
Procedural Best Practices for Total Fiberoptic Colonoscopy
Bowel Preparation
Thorough mechanical cleansing is non-negotiable. ESGE 2019 guidelines recommend split-dose preparation — the last dose starting within 5 hours of the procedure and finishing at least 2 hours prior. Accepted regimens include high-volume 4L PEG or low-volume 2L PEG-based solutions, combined with a low-fiber diet the day before.
Inadequate preparation has concrete consequences:
- Higher adenoma miss rate, including a threefold higher miss rate for adenomas ≥5 mm per ESGE guidance
- Increased cecal intubation failure
- Prolonged procedure time and greater technical difficulty
Loop Management
Looping in the sigmoid and transverse colon accounts for roughly 50% of incomplete procedures. The fundamental technique: withdraw and straighten the scope rather than advancing through a loop. Pushing forward through an unresolved loop amplifies patient discomfort and reduces tip control.
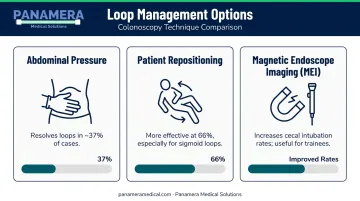
Practical management options:
- Abdominal pressure — resolves loops in approximately 37% of cases
- Patient repositioning — more effective at 66%, particularly for sigmoid loops
- Magnetic endoscope imaging (MEI) — increases cecal intubation rates and reduces time, especially useful for trainees
Patient Positioning and Sedation
Most procedures start in the left lateral (Sims') position. Repositioning to supine or right lateral during the transverse colon phase often helps with loop reduction and hepatic flexure navigation.
Sedation selection follows positioning decisions. ASGE defines moderate sedation as maintaining purposeful response to stimulation — the standard for most colonoscopies. Anesthesia-provider involvement is appropriate when any of the following apply:
- Severe comorbidities (ASA IV/V)
- Anticipated intolerance to standard sedatives
- Deep sedation is planned
CO₂ Insufflation
The shift from air to carbon dioxide insufflation is one of the clearest evidence-based upgrades in colonoscopy technique. A meta-analysis of 21 RCTs found CO₂ significantly increased the proportion of patients without pain at 1 hour post-procedure (RR 1.84; 95% CI 1.37–2.47) and at 6 hours (RR 1.28; 95% CI 1.14–1.44), with no significant change in blood CO₂ levels.
For facilities still using room air, the switchover requires only a compatible CO₂ insufflator — hardware now standard across Olympus, Pentax, and Fujifilm endoscopy platforms.
Fiberoptic vs. Video Colonoscopes: Clinical and Equipment Considerations
Image Quality and Documentation
The practical difference comes down to where image capture happens:
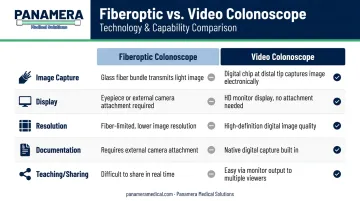
| Feature | Fiberoptic | Video (CCD/CMOS) |
|---|---|---|
| Image capture location | Glass fiber bundle → eyepiece | Digital chip at distal tip |
| Display | Eyepiece or external camera head | Direct to HD monitor |
| Resolution | Limited by fiber diameter and bundle density | High-definition digital |
| Documentation | Requires external camera attachment | Native digital capture |
| Teaching/sharing | Difficult in real time | Easy via monitor output |
No peer-reviewed study has directly compared adenoma detection rates between legacy fiberoptic scopes and modern video systems in a head-to-head trial. What is documented is that high-definition video colonoscopy shows a 3.5% incremental yield for adenomatous polyps compared with standard-definition video endoscopy — the video generation itself was the step change in detection capability.
Where Fiberoptic Scopes Remain Relevant
Fiberoptic colonoscopes continue to serve a functional role in several scenarios:
- A 2024 survey of Pacific Island endoscopy sites found facilities averaging just four functional endoscopes, with 75% sending instruments overseas for repair — in these resource-limited environments, keeping any functional colonoscope operational is a priority
- When video scopes are out for repair, a fiberoptic scope keeps the endoscopy schedule running without canceling cases
- Pre-video generation equipment can serve as a workable entry point for facilities not yet ready for full video system investment
When a facility does reach the point of transitioning away from fiberoptic equipment, aging inventory doesn't have to be a sunk cost. Panamera Medical Solutions' buy-back and trade-in programs allow facilities to recover value from fiberoptic scopes, applying that credit toward current-generation video colonoscopes such as the Olympus CF-HQ190, Pentax EC-38-i10L, or Fujifilm EC-760R-V/L, along with compatible processors like the Olympus CV-190 or Fujifilm VP-7000.
Fiber Breakage and Image Degradation
Fiberoptic bundle degradation is cumulative and irreversible. Each broken fiber becomes a permanent black dot in the image field. As the count grows, the clinical image becomes progressively less reliable for detecting flat lesions or subtle mucosal changes. At that point, the scope is signaling both a clinical and a financial problem: repair costs on a bundle with severe fiber loss will recur, while image quality continues to decline regardless of servicing.
Reprocessing, Maintenance, and Equipment Lifecycle Management
Reprocessing Requirements
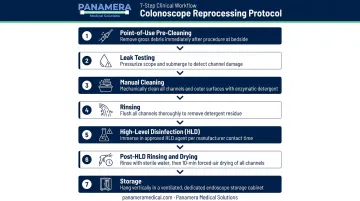
High-level disinfection (HLD) is the minimum standard for fiberoptic colonoscopes between procedures. The reprocessing sequence follows CDC/HICPAC and SGNA guidance:
- Point-of-use pre-cleaning — remove gross debris immediately after withdrawal
- Leak testing — before manual cleaning, per manufacturer IFU; detects damage to channels and exterior
- Manual cleaning — enzymatic detergent, brushing and flushing all channels
- Rinsing — thorough water rinse post-cleaning
- HLD — automated endoscope reprocessor (AER) or manual soaking with validated disinfectant at minimum effective concentration
- Post-HLD rinsing and drying — AAMI ST91:2021 recommends minimum 10-minute forced-air drying with pressure-regulated air through each channel
- Storage — vertical hanging in a ventilated cabinet; avoid tight coiling
For fiberoptic scopes specifically, manual cleaning requires careful handling. Harsh bending during cleaning accelerates fiber breakage, damaging the instrument in the same process meant to preserve it.
Preventive Maintenance and Storage
Routine preventive maintenance extends scope lifespan. A 2024 study found that implementing borescope inspections reduced major repairs from 12.1% to 3.2% and cut mean repair costs from $4,426 to $2,337 — nearly a 40% reduction in total annual repair expenditure.
Key PM practices for fiberoptic colonoscopes:
- Leak test before every procedure session, not just periodically
- Store vertically, hanging straight — coiling tightens the insertion tube and stresses fiber bundles
- Avoid sharp bends during transport and storage
- Schedule periodic inspection by a qualified biomedical technician
- Document repair history per scope to track cumulative costs over time
Equipment Lifecycle Decision-Making
That repair history documentation feeds directly into the repair vs. replace decision. The inflection point comes down to two converging signals: cumulative repair costs and image quality. Neither alone is definitive, but together they mark when continued investment stops making sense.
A fiberoptic colonoscope with significant fiber breakage, recurrent channel leaks, or angulation wire issues may accumulate repair costs that approach or exceed the value of a refurbished video replacement. At that point, continued investment in the old scope is a poor return.
Panamera Medical Solutions offers both buy-back and trade-in options for facilities managing aging colonoscope inventories. The buy-back program provides direct cash payment for decommissioned equipment; the trade-in program applies the value as credit toward upgraded video systems. Both options are available across their network spanning North America, Europe, and South America.
Frequently Asked Questions
What is a fiberoptic colonoscopy?
A fiberoptic colonoscopy is a procedure that uses a flexible colonoscope containing bundled glass fibers to visualize the entire large intestine. It allows both diagnosis and treatment — including biopsy and polyp removal — within the same session, without surgery.
What type of doctor performs a colonoscopy?
Colonoscopies are typically performed by gastroenterologists or colorectal surgeons, and in some settings by trained general surgeons or advanced endoscopy fellows.
Why are colonoscopies more difficult in women?
Anatomical differences — including a longer colon on average, a more mobile mesocolon, and the effects of prior pelvic surgeries or adhesions — increase the likelihood of sigmoid loop formation in women. This often requires additional technique adjustments such as repositioning or abdominal compression.
What is the difference between a fiberoptic and a video colonoscope?
Fiberoptic colonoscopes carry images optically through glass fiber bundles to an eyepiece or external camera head. Video colonoscopes embed a digital CCD or CMOS chip at the distal tip, transmitting high-definition images directly to a monitor. This delivers superior resolution and simpler documentation.
How long does a fiberoptic colonoscopy take?
A fiberoptic colonoscopy typically takes 20 to 60 minutes, depending on bowel preparation quality, patient anatomy, and whether therapeutic interventions are performed. Skilled operators routinely complete diagnostic cases in 20–30 minutes.
Can a fiberoptic colonoscope be used for therapeutic procedures?
Yes. Any fiberoptic colonoscope with a working channel supports therapeutic interventions including polypectomy, biopsy, hemostasis, and injection therapy — making a single procedure both diagnostic and therapeutic when indicated.