This overview explains what flexible bronchoscopy is, how it works, where it applies, what affects outcomes, and when it is not the right choice.
Key Takeaways
- Flexible bronchoscopy enables direct visualization of the trachea, bronchi, and distal airways without general anesthesia
- It serves both diagnostic (tissue sampling, BAL) and therapeutic (secretion clearance, foreign body removal, stenting) functions
- The procedure runs in outpatient, inpatient, and ICU settings, including on ventilated patients
- Outcomes depend heavily on equipment quality, operator experience, and pre-procedure preparation
- Key differences from rigid bronchoscopy span access route, sedation requirements, and clinical applications
What Is Flexible Bronchoscopy and Why Is It Used in Adults?
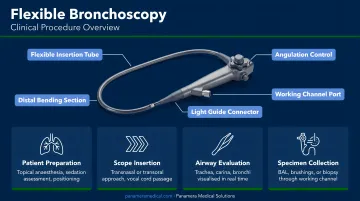
Flexible bronchoscopy uses a slender, steerable endoscope passed through the nose or mouth, past the vocal cords, and into the tracheobronchial tree. This allows direct visual inspection, specimen collection, and treatment delivery — all without surgical access.
The goal is real-time examination of central and peripheral airways, enabling accurate diagnosis and targeted therapy in a single procedure.
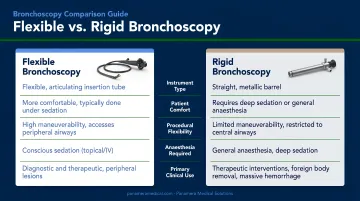
How It Differs from Rigid Bronchoscopy
| Feature | Flexible | Rigid |
|---|---|---|
| Anesthesia required | Topical + moderate sedation | General anesthesia |
| Airway access | Central and distal | Central only |
| Portability | Yes — bedside capable | No — OR only |
| Instrument size | Limited by working channel | Larger instruments possible |
| Best for | Diagnosis, BAL, routine therapy | Massive hemorrhage, large foreign bodies |
Clinical Standing
The British Thoracic Society's NICE-accredited guideline establishes flexible bronchoscopy as the standard of care for a broad set of indications. The 2019 ICS/NCCP(I)/IAB adult guideline maps these explicitly:
- Hemoptysis and unexplained radiographic abnormalities
- Persistent cough or suspected airway malignancy
- Lung cancer staging and pulmonary infiltrates
- Airway collapse, localized wheeze, and stridor
More than 500,000 flexible bronchoscopies are performed annually in the US, according to an ACCP/AAB consensus statement. In US hospitals, the procedure appeared in over 609,000 invasive mechanical ventilation hospitalizations between 2012 and 2018 — with adoption climbing from 9.5% to 10.8% across that period.
How Flexible Bronchoscopy Works: Equipment and Procedure
Bronchoscope Types
Three scope types are used in adult practice:
- Fiberoptic — image transmitted via fiberoptic bundles to a proximal eyepiece or attached camera; lower cost, smaller diameter options available
- Video/chip-tip — CCD chip at the distal tip captures a digital image transmitted electronically; higher resolution, higher cost
- Hybrid — combines a fiberoptic image bundle with a distal CCD chip
Video bronchoscopes offer superior image quality for complex procedures. Fiberoptic devices provide practical advantages where diameter or cost matters.
Key Physical Specifications
Adult flexible bronchoscopes share a working length of approximately 600 mm, with distal outer diameters ranging from around 3.0 mm (ultrathin, such as the Olympus BF-XP190) to 5.8 mm (therapeutic, such as the Fujifilm EB-710XT). Working channel sizes run from 1.2 mm to 3.2 mm depending on model.
Larger channels support better secretion clearance but reduce maneuverability in distal airways.
The working channel also passes biopsy forceps, cytology brushes, and needles, and connects to suction controlled at the handle — making the scope functional for both sampling and treatment in one pass.
Preparing the Patient
Pre-procedure steps include:
- Patient fasting (typically 4–6 hours for solids)
- Medication review — anticoagulants, antiplatelets, and diabetic agents require specific management
- Baseline vitals, IV access, and pre-oxygenation
- Informed consent after explaining risks, benefits, and alternatives
Airway Anesthesia and Scope Insertion
The airway is anesthetized using topical lidocaine spray applied to the nose or mouth, throat, vocal cords, and trachea. IV moderate sedation (midazolam and fentanyl are the preferred agents per ACCP consensus) is added to reduce discomfort and suppress the cough reflex.
The bronchoscope is introduced transnasally or transorally, navigated past the vocal cords, and advanced through the bronchial tree using tip angulation and rotational torque.
Inspection, Sampling, and Intervention
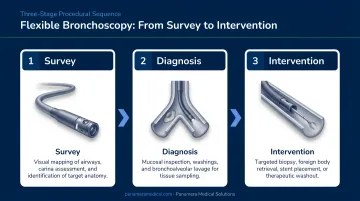
Once positioned, the procedural sequence is:
- Systematic survey — vocal cords, trachea, carina, bilateral bronchial segments
- Specimen collection — biopsies via forceps, brushings via cytology brush, washings or BAL via saline instillation and suction
- Therapeutic actions — secretion clearance, hemostasis, or device placement as indicated
Scope maintenance, sterilization compliance, and working channel integrity all affect procedural safety and image quality. Facilities managing aging or high-utilization bronchoscope fleets — models like the Olympus BF-1TH190 or Pentax EB19-J10 are common candidates — often evaluate trade-in or equipment replacement options. Panamera Medical Solutions works with hospitals and endoscopy programs on used and refurbished bronchoscope sourcing and trade-ins across North America, Europe, and South America.
Diagnostic and Therapeutic Applications in Adults
Diagnostic Indications
- Investigation of hemoptysis
- Evaluation of persistent or unexplained cough
- Assessment of radiographic abnormalities — masses, infiltrates, nodules
- Staging and sampling of suspected lung malignancy
- Diagnosis of infections (BAL for pneumonia; fungal workup in immunocompromised patients)
- Assessment of airway burns or inhalation injury
- Evaluation of collapse, localized wheeze, or stridor
BAL diagnostic yield in immunocompromised adults reaches 52.4% in elective settings. In non-HIV immunocompromised ICU patients, yield drops to roughly 33% — but that figure holds clinical weight when results directly change antimicrobial management.
Therapeutic Indications
- Clearance of thick secretions or mucus plugging, most often in ICU patients
- Control of endobronchial bleeding
- Foreign body removal
- Guidance for percutaneous tracheostomy
- Placement of endobronchial valves or blockers
- Facilitation of difficult intubation (awake fiberoptic intubation)
Procedure Complexity Tiers
| Tier | Procedures | Notes |
|---|---|---|
| Routine | Inspection, BAL, endobronchial biopsy | Performed by most pulmonologists |
| Advanced | Transbronchial biopsy, TBNA | Higher complexity; additional training needed |
| Specialized | Laser resection, stenting, EBUS | Requires subspecialty expertise |
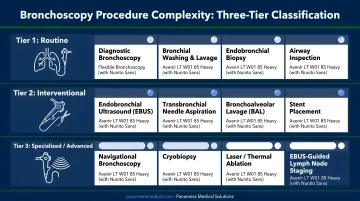
Complication risk scales with procedural complexity. A routine BAL in a stable patient is a low-stakes procedure; a transbronchial biopsy in a coagulopathic patient on mechanical ventilation is not — and pre-procedure planning should reflect that difference.
Factors That Affect Bronchoscopy Outcomes
Patient-Related Factors
- Baseline respiratory reserve and resting oxygen saturation
- Cardiac status — elective bronchoscopy should be deferred within 4–6 weeks of acute myocardial infarction
- Coagulation profile — uncorrected coagulopathy is a contraindication when biopsies are planned
- Whether the patient is spontaneously breathing or intubated
Absolute contraindications per the 2019 ICS/NCCP(I)/IAB guideline include lack of informed consent, absence of a trained bronchoscopist, profound refractory hypoxemia, and severe uncorrectable bleeding diathesis.
Equipment and Operator Factors
Scope diameter selection relative to the target airway, image system quality, and working channel size for the planned procedure all affect what is achievable. Operator experience directly affects both complication rates and procedure time.
A prospective study of 967 flexible bronchoscopies found a 4.5% complication rate when trainees were involved versus 1.2% without. Mean procedure time was also longer: 50.8 minutes with trainees versus 32.5 minutes without.
The ICS/NCCP(I)/IAB guideline recommends a minimum of 25 procedures per year to maintain competency.
Procedural and Environmental Factors
- Inadequate airway anesthesia (insufficient lidocaine) increases cough, bronchospasm, and scope movement
- In intubated patients, increase FiO2 to 1.0 before and during the procedure; volume-controlled ventilation modes are preferred
- Monitor continuously: SpO2, tidal volume, peak inspiratory pressure, and FiO2 throughout; resuscitation equipment must be immediately available
Misconceptions and When Flexible Bronchoscopy May Not Be Appropriate
Misconception 1: Flexible and Rigid Bronchoscopy Are Interchangeable
They are not. Rigid bronchoscopy is the appropriate tool for:
- Massive hemorrhage — rigid provides airway control and suction capacity that flexible bronchoscopy cannot match
- Large foreign body retrieval — the larger working barrel and extraction instruments are necessary for selected objects
- Significant airway stenosis — rigid allows dilation and stenting with tools that exceed flexible scope capabilities
Flexible bronchoscopy is not a universal substitute for rigid bronchoscopy. When the clinical situation calls for rigid bronchoscopy, substituting a flexible scope delays definitive intervention and can worsen outcomes.
Misconception 2: Complications Are Too Rare to Warrant Rigorous Monitoring
Major complications are infrequent but not negligible. A prospective cooperative study of 908 patients reported a 1.7% major complication rate and 0.1% mortality. A 2015 synopsis of published bronchoscopy literature reports:
- Respiratory failure / severe hypoxia: 0.2–0.31%
- Bronchospasm / laryngospasm: 0.26–2%
- Hemorrhage >50 mL: 0.12–0.17%
- Post-bronchoscopy infectious fever: approximately 3.5%
These rates apply to routine diagnostic procedures — high-risk biopsy cohorts show adverse event rates as high as 35%, with severe events in 10%. Active monitoring protocols are not optional.
When Flexible Bronchoscopy Is Not the Right First Choice
- Uncorrected coagulopathy when biopsies are planned
- Severe respiratory failure without intubation
- Large-lumen interventions best suited to rigid bronchoscopy
- Peripheral lesions where CT-guided biopsy offers better yield
For peripheral pulmonary nodules, the yield gap is significant. CT-guided transthoracic needle biopsy achieves sensitivity of ≥90% for malignancy, while fluoroscopy-guided transbronchial biopsy reaches only 31% median sensitivity for nodules under 2 cm.
Navigation bronchoscopy and radial EBUS improve on standard transbronchial biopsy for peripheral lesions, but CT guidance remains the stronger option in selected cases.
Frequently Asked Questions
How long does a flexible bronchoscopy take?
The procedure itself typically takes 20–30 minutes, though total encounter time including preparation and recovery extends to approximately 1–2 hours. Therapeutic or technically complex cases run longer than purely diagnostic ones.
What is a flexible bronchoscope used for?
Flexible bronchoscopes serve both diagnostic and therapeutic purposes:
- Diagnostic: airway inspection, tissue biopsy, bronchoalveolar lavage (BAL) for infection or cytology
- Therapeutic: secretion clearance, foreign body removal, hemostasis, endobronchial valve placement, and guidance for percutaneous tracheostomy or difficult intubation
What is the difference between a rigid and flexible bronchoscope?
Flexible bronchoscopes are thin and steerable, used under topical anesthesia or moderate sedation, which allows access to distal airways. Rigid bronchoscopes are straight metal tubes that require general anesthesia but offer a larger working lumen and better airway control — making them preferable for massive hemorrhage or foreign body retrieval.
What type of anesthesia is used for flexible bronchoscopy in adults?
Most adult procedures use topical lidocaine applied to the airway combined with IV moderate sedation (typically midazolam and fentanyl, per ACCP consensus recommendations). General anesthesia is not routinely required.
Can flexible bronchoscopy be performed on mechanically ventilated patients?
Yes. The bronchoscope is inserted through a Y-connector attached to the ventilator circuit. FiO2 should be increased to 1.0 before and during the procedure. Ventilator settings — mode, tidal volume, and inspiratory flow — require adjustment to compensate for the partial airway obstruction the scope creates.