Speed and precision matter. And that's exactly where endoscopic ultrasound (EUS) earns its place at the front of the diagnostic workup.
EUS combines high-resolution ultrasound imaging with real-time tissue sampling in a single procedure — positioning the transducer millimeters from pancreatic tissue through the stomach or duodenum wall. No external imaging modality gets that close. For clinicians managing a suspected pancreatic mass, EUS is the tool that turns a suspicious finding into an actionable diagnosis.
Key Takeaways
- EUS positions the ultrasound transducer closer to the pancreas than any external imaging, detecting masses CT and MRI miss.
- EUS-guided FNA/FNB enables simultaneous imaging and tissue acquisition in one session.
- For potentially resectable masses, EUS is preferred over percutaneous CT-guided biopsy due to far lower peritoneal seeding risk.
- The procedure typically takes under an hour under moderate sedation, with an overall complication rate under 1%.
- Diagnostic accuracy depends on operator expertise and equipment; linear array echoendoscopes are required for tissue sampling.
What Is Endoscopic Ultrasound (EUS)?
EUS is a minimally invasive procedure combining a flexible endoscope with a high-frequency ultrasound transducer mounted at its tip. The scope is inserted orally and advanced through the esophagus and stomach — or into the duodenum — placing the transducer directly against the GI tract wall, immediately adjacent to the pancreas.
Two Clinically Relevant Modalities
EUS operates in two distinct modes depending on clinical need:
- Diagnostic EUS (imaging only): assesses pancreatic morphology, echogenicity, borders, vascularity, and locoregional staging
- Interventional EUS: adds FNA (fine needle aspiration for cytology) or FNB (fine needle biopsy for histological core tissue), enabling tissue confirmation during the same session
The distinction has direct equipment implications. Tissue acquisition requires a linear array echoendoscope, where the needle path stays within the ultrasound imaging plane and can be visualized in real time. Radial echoendoscopes produce high-quality cross-sectional images but cannot guide needle passes safely.
What Patients Experience
Understanding the procedure's technical scope helps set appropriate patient expectations. EUS is performed in an outpatient or same-day surgery setting, with patients receiving moderate sedation — most report minimal discomfort. Diagnostic cases typically run under an hour; interventional EUS with FNA/FNB may run slightly longer.
Why EUS Is the Preferred Method for Diagnosing Pancreatic Masses
Anatomical Proximity Translates to Resolution
The pancreas sits directly behind the posterior gastric wall and within millimeters of the duodenum. An EUS transducer operating at 7.5–20 MHz from inside the stomach wall can resolve pancreatic structures as small as 2–3 mm — detail that external imaging simply cannot match across the abdominal wall.
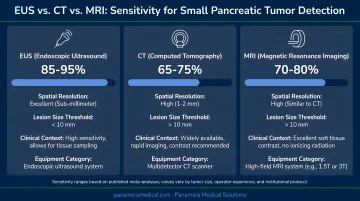
Superior Detection of Small Lesions
This matters most for small tumors, where early diagnosis is still possible. A comparison published in Radiology found:
| Modality | Sensitivity for masses <3 cm | Specificity |
|---|---|---|
| EUS | 93% | 100% |
| MRI | 67% | — |
| CT | 53% | 64% |
For tumors under 20 mm specifically, EUS sensitivity reaches 94.4% versus 50% for contrast-enhanced CT. That gap is the difference between a resectable tumor caught early and one missed entirely.
Tissue Diagnosis in One Procedure
Rather than ordering a separate biopsy after initial imaging, EUS-FNA or EUS-FNB delivers cytological or histological material during the same session. Pathology can confirm malignancy, subtype the tumor, and provide material for molecular profiling — all without an additional procedure.
Subtypes identified include pancreatic ductal adenocarcinoma, neuroendocrine tumor, lymphoma, and metastatic lesions. The ASGE 2024 guidelines now recommend FNB over FNA for solid pancreatic masses, particularly when molecular testing is anticipated.
Locoregional Staging Built In
While imaging the mass, the endosonographer simultaneously evaluates:
- Portal vein involvement
- Proximity to the superior mesenteric artery and vein
- Peripancreatic lymph node status
- Bile duct involvement
This locoregional staging data directly informs resectability classification — without requiring a separate imaging session.
Lower Peritoneal Seeding Risk
For potentially resectable masses, how tissue is obtained carries oncological consequences. Micames et al., published in Gastrointestinal Endoscopy, reported peritoneal carcinomatosis in 2.2% of patients biopsied via EUS-FNA versus 16.3% after percutaneous CT/US-guided FNA. EUS avoids crossing the peritoneal cavity entirely, eliminating the needle-track seeding pathway that percutaneous routes carry.
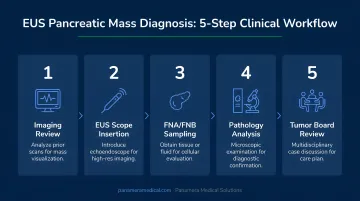
How EUS Diagnoses Pancreatic Masses: A Step-by-Step Breakdown
EUS may appear to be a single procedure, but accurate pancreatic mass diagnosis involves a structured clinical workflow. Each stage — from imaging review to tumor board synthesis — directly affects diagnostic accuracy.
Step 1 – Pre-Procedure Imaging Review
EUS follows initial detection on CT or MRI. The endosonographer reviews prior imaging to identify the target location (head, body, or tail), estimate mass size, and assess vascular involvement that could complicate needle access.
Step 2 – Patient Preparation
- Fasting: NPO for at least 6 hours before the procedure
- Medications: Anticoagulants and antiplatelet agents require management per bridging protocols
- Sedation planning: Moderate sedation for most cases; monitored anesthesia care for complex procedures
- Consent: Must include specific FNA/FNB risks — pancreatitis, bleeding, infection, perforation
Step 3 – Scope Insertion and Imaging
The linear array echoendoscope is advanced to the stomach (body/tail lesions) or duodenum (head/uncinate lesions). The endosonographer systematically scans the pancreas, characterizing the mass's echogenicity, borders, internal architecture, and vascular relationships.
Step 4 – FNA or FNB Tissue Acquisition
Under real-time EUS guidance, a needle is advanced through the scope's working channel into the mass. ESGE recommends 22G or 25G for routine sampling; 19G FNA/FNB or 22G FNB when a histologic core is needed. Multiple passes are typically made.
- FNA: Collects loose cells for cytological analysis
- FNB: Retrieves intact core tissue for histology and molecular profiling
On-site cytopathology (ROSE) can improve adequacy assessment, though ASGE 2024 advises against making it routine for initial EUS tissue acquisition.
Step 5 – Pathology and Staging Synthesis
Once acquisition is complete, the lab processes samples as cytology smears, cell blocks, or core biopsies. For PDAC molecular testing, FNB significantly outperforms FNA: one 2024 study found molecular-test adequacy of 71.4% with FNB versus 32.1% with FNA.
EUS findings are then integrated with CT/MRI data in a multidisciplinary tumor board. That synthesis classifies the mass as resectable, borderline resectable, locally advanced, or metastatic, determining whether the patient proceeds to surgery, neoadjuvant therapy, or palliative care.
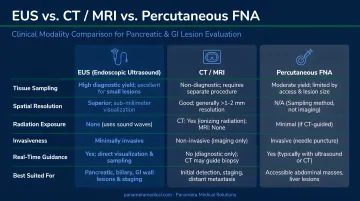
EUS vs. CT, MRI, and Percutaneous FNA: A Clinical Comparison
| Feature | EUS | CT | MRI | Percutaneous FNA |
|---|---|---|---|---|
| Sensitivity for masses <3 cm | 93–94% | 50–53% | 67% | Variable |
| Same-session tissue acquisition | Yes | No | No | Yes (separate procedure) |
| Peritoneal seeding risk | ~2.2% | N/A | N/A | ~16.3% |
| Radiation exposure | None | 11–15 mSv (median) | None | Guided by CT (radiation) |
| Locoregional vascular staging | High detail | Good | Good | Limited |
| Distant metastasis assessment | Limited | Excellent | Excellent | N/A |
When Each Modality Leads
- CT/MRI leads for initial mass detection, gross resectability assessment, and whole-abdomen staging (liver or peritoneal metastases). EUS cannot replace these modalities for distant disease.
- EUS steps in when tissue diagnosis is needed, when CT cannot characterize a small lesion, or when vascular assessment detail changes the resectability call.
- Percutaneous FNA is reserved for unresectable masses, surgically altered anatomy that limits EUS access, or settings where EUS is unavailable.
EUS as a Salvage Diagnostic Tool
When percutaneous biopsy fails, EUS-FNA remains effective. Published data show EUS-FNA achieving approximately 90% sensitivity in pancreatic malignancy diagnosis after previously negative CT-guided biopsies, confirming its value as a reliable second-line option when initial percutaneous attempts are non-diagnostic.
Risks, Limitations, and What Patients Should Expect
EUS with FNA/FNB is well-tolerated, though patients should understand its risk profile before the procedure.
Complication Rates
A systematic review of over 10,900 EUS-FNA procedures found:
- Overall morbidity: 0.98%
- Acute pancreatitis: 0.44% (solid lesions); up to 1.8% in some cohorts
- Cyst infection: 0.2%
- Bleeding: ~0.3% in solid-lesion series
- Perforation: Recognized but rare; no reliable separate rate for solid pancreatic lesions
Cystic lesions carry a higher complication rate (2.75%) than solid masses (0.82%).
Special Considerations
- Surgically altered anatomy (post-Whipple, Roux-en-Y gastric bypass): EUS access may be limited or impossible; percutaneous approaches may be preferred
- Anticoagulation: Requires bridging protocols before FNA/FNB
- High anesthesia risk: Consider percutaneous alternatives when sedation poses excessive risk
Recovery Expectations
- Recovery time: Most patients are discharged within a few hours
- Common side effects: Mild bloating or gas, resolving quickly
- Sedation: Effects clear within 30–60 minutes; patients need a driver and should avoid critical decision-making for the remainder of the day
- Pathology turnaround: Results typically return within 3–7 days
How Panamera Medical Solutions Can Help
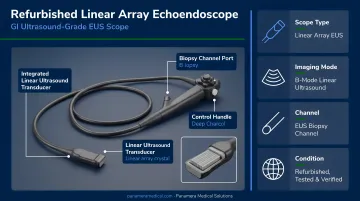
Diagnostic accuracy in EUS isn't only about operator skill — the echoendoscope itself matters. A high-resolution linear array scope is required for FNA/FNB, and aging or underperforming equipment directly compromises both lesion detection and tissue yield. GI units and cancer centers running older platforms are carrying a clinical performance gap that's often avoidable.
Panamera Medical Solutions works with healthcare facilities across North America, Europe, and South America to source, sell, and service pre-owned and refurbished endoscopic equipment, including linear array echoendoscopes such as the Olympus GF-UCT180, a curved linear array ultrasound endoscope designed for advanced diagnostic and therapeutic GI procedures.
For facilities looking to upgrade their EUS capability without absorbing the full cost of new equipment, Panamera's Trade-In and Buy-Back programs offer a practical path forward:
- Equipment Credit (Trade-In): Apply the value of older echoendoscopes toward a newer-generation platform
- Cash Recovery (Buy-Back): Convert unused or decommissioned scopes into cash through Panamera's global buyer network
Older equipment often retains value to international buyers that domestic facilities can't access independently. With over 15 years of global trading experience, Panamera connects GI units with motivated buyers across continents — reducing upfront costs on the upgrade side.
For facilities where EUS volume or pancreatic diagnostic workload is growing, that freed-up capital can go directly toward higher-performing equipment rather than sitting in decommissioned inventory.
Frequently Asked Questions
Is a pancreatic mass usually cancer?
Not automatically. While pancreatic ductal adenocarcinoma accounts for 85–90% of malignant pancreatic tumors, solid masses can also represent neuroendocrine tumors, autoimmune pancreatitis, or metastatic deposits. Tissue diagnosis is essential, not assumed, because benign mimics exist and treatment differs significantly.
Can EUS detect pancreatic cancer?
Yes, and it's among the most sensitive tools available. EUS achieves 93% sensitivity for tumors under 3 cm versus 53% for CT. It also enables same-session tissue sampling to confirm the diagnosis, making it the preferred next step after equivocal or non-diagnostic cross-sectional imaging.
What are the risks of EUS with FNA?
Complications are uncommon. The most frequent is acute pancreatitis (under 0.5% in most series), with bleeding, infection, and perforation occurring rarely. Peritoneal seeding risk is dramatically lower than with percutaneous CT-guided biopsy (2.2% vs. 16.3%), making EUS the safer route for potentially resectable lesions.
How painful is a pancreatic biopsy via EUS?
Patients receive moderate sedation or monitored anesthesia care, so discomfort during the procedure is minimal for most. Mild bloating or gas afterward is common and typically resolves within hours. Significant post-procedure pain is unusual.
How accurate is EUS-FNA for diagnosing pancreatic cancer?
A meta-analysis reported pooled sensitivity of 88.6% and specificity of 99.3% for pancreatic ductal adenocarcinoma. Diagnostic yield improves further with experienced operators and, selectively, with on-site cytopathology (ROSE) when local adequacy assessment is needed.
What is the difference between EUS-FNA and EUS-FNB?
FNA collects loose cells via thin needles for cytological review; FNB uses core-biopsy needles to retrieve intact tissue fragments for histological analysis. ASGE 2024 guidelines recommend FNB for solid pancreatic masses, especially when molecular profiling or next-generation sequencing is planned, as FNB delivers adequate tissue for genomic testing at more than twice the rate of FNA.