The confusion is understandable. Both procedures use an endoscope. Both visualize the same anatomical territory. But one is built for seeing, the other for doing — and that distinction shapes every clinical decision downstream.
This article breaks down how each procedure works, where they diverge, and the specific clinical situations where one clearly outperforms the other.
Key Takeaways
- EUS delivers high-resolution imaging and tissue sampling via ultrasound waves
- ERCP combines endoscopy with fluoroscopy for direct ductal intervention — used when treatment is confirmed necessary
- EUS is the safer first-line option when the diagnosis remains uncertain
- Post-ERCP pancreatitis occurs in 3–10% of procedures — a risk EUS does not carry
- An "EUS-first" strategy in intermediate-risk patients significantly cuts unnecessary ERCP referrals
- Both procedures can be performed in the same session at tertiary care centers when clinically appropriate
EUS vs ERCP: Quick Comparison
The table below summarizes how EUS and ERCP differ across the criteria that matter most when selecting the right procedure for a patient.
| Feature | EUS | ERCP |
|---|---|---|
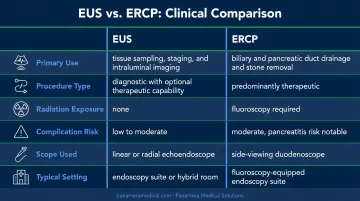
| Primary purpose | Diagnostic — imaging, staging, biopsy | Therapeutic — ductal intervention |
| Imaging method | High-frequency ultrasound through GI wall | Fluoroscopy with contrast dye injection |
| Scope type | Linear-array or radial-array echoendoscope | Side-viewing duodenoscope |
| Risk profile | Low; most complications are mild | Higher; post-procedural pancreatitis in 3–10% |
| Key clinical uses | Pancreatic masses, cyst evaluation, cancer staging, FNA/FNB, celiac plexus blocks | Bile duct stone removal, stent placement, sphincterotomy, stricture dilation |
| Tissue sampling | Yes — via FNA or FNB needle guidance | Limited — brushings or forceps biopsy only |
What Is Endoscopic Ultrasound (EUS)?
EUS passes a specialized echoendoscope — fitted with an ultrasound transducer at its tip — through the mouth and into the stomach or duodenum. At that close range, sound waves pass through the GI wall to generate real-time images of the pancreas, bile ducts, liver, gallbladder, lymph nodes, and adjacent vasculature. No radiation. No contrast dye.
Two Scope Subtypes
- Radial-array EUS: generates a 360-degree panoramic view perpendicular to the endoscope axis; the standard choice for staging
- Linear-array EUS: generates a single-plane image parallel to the axis, enabling real-time needle guidance for FNA/FNB; increasingly dominant given its therapeutic versatility
For interventional procedures — drainage, celiac plexus blocks, biliary access — a linear echoendoscope is required.
Clinical Applications
EUS covers a broad range of diagnostic and therapeutic indications:
- Pancreatic mass evaluation and biopsy (EUS-FNA/FNB)
- GI cancer staging (esophageal, gastric, rectal, pancreatic)
- Pancreatic cyst characterization (benign vs. malignant)
- Bile duct stone detection
- Pseudocyst drainage
- Celiac plexus neurolysis for pain management in pancreatic cancer
Detection Accuracy
The sensitivity numbers are compelling. A systematic review published by Kitano et al. found median EUS sensitivity for pancreatic tumors at 94%, compared to 74% for CT across 22 studies and 1,170 patients. For bile duct stones specifically, ESGE data reports EUS sensitivity at 95% with specificity of 97% — marginally outperforming MRCP.
EUS-FNA adds another layer: pooled data from Chen et al. shows 90.8% sensitivity and 96.5% specificity for pancreatic masses, making it the most accurate non-surgical tissue sampling method available.
Safety Profile
EUS carries a low complication burden. Large systematic review data puts the EUS-FNA total complication rate at 0.98%, with mortality at 0.02%. Diagnostic EUS perforation risk sits around 0.02%. The most frequent patient complaints are sore throat, bloating, and mild sedation effects — far milder than the complication profile associated with ERCP.
U.S. upper EUS volumes increased more than sixfold in some age groups between 2002 and 2019, driving sustained demand for linear echoendoscopes. Facilities expanding EUS programs can offset upgrade costs through equipment trade-in options. Panamera Medical Solutions carries the Olympus GF-UCT180 curved linear array echoendoscope and offers buy-back programs for older scopes being phased out.
What Is ERCP?
ERCP advances a side-viewing duodenoscope to the duodenum, where the physician cannulates the ampulla of Vater. Contrast dye is injected into the ducts, and fluoroscopy reveals obstructions, stones, strictures, or leaks. Instruments pass through the working channel immediately, so diagnosis and treatment happen in the same session — that dual function is what keeps ERCP essential for ductal intervention.
Core Therapeutic Capabilities
- Biliary sphincterotomy
- Bile duct stone extraction (choledocholithiasis)
- Biliary or pancreatic stent placement
- Stricture balloon dilation
- Tissue sampling via brushings or biopsy forceps
- Post-surgical bile duct leak repair
The Diagnostic vs. Therapeutic Distinction
This distinction matters clinically and is often misunderstood. Diagnostic ERCP — using the procedure purely to visualize ducts — has largely been replaced by MRCP and EUS in most protocols. Both offer comparable accuracy without ERCP's complication risk. What remains firmly in ERCP's domain is therapeutic ERCP: interventions that simply cannot be performed any other way.
Risk Profile
ERCP carries a notably higher complication burden than most endoscopic procedures:
| Complication | Incidence |
|---|---|
| Post-ERCP pancreatitis (overall) | 3–10% |
| Post-ERCP pancreatitis (high-risk patients) | Up to 14.7% |
| Postsphincterotomy bleeding | 0.3–2% |
| Cholangitis | 0.5–3% |
| Duodenal perforation | 0.08–0.6% |
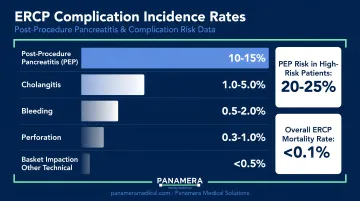
PEP mortality is rare but documented at 0.1–0.7%. Risk increases substantially in younger patients, those with normal bilirubin, suspected sphincter of Oddi dysfunction, difficult cannulation, and lower-volume centers.
For facilities running active ERCP programs, duodenoscope selection and maintenance are operationally significant. The Olympus TJF-Q190V is one of the models Panamera Medical Solutions trades and services, which can be useful context for procurement teams evaluating equipment upgrades or lifecycle planning.
EUS vs ERCP: Which Procedure Is Right for the Patient?
The core question is simple: Is the clinical goal diagnostic or therapeutic?
If diagnostic — EUS. If therapeutic and confirmed — ERCP. If uncertain — EUS first.
When to Choose EUS
- A pancreatic or biliary mass needs characterization or tissue diagnosis
- Cancer staging is required before treatment planning
- A patient has intermediate probability of bile duct stones (10–50% probability per ASGE) and it's unclear whether ERCP is warranted
- CT or MRI results are inconclusive
- A pseudocyst requires drainage
- ERCP has failed and biliary access is still needed (EUS-guided biliary drainage)
When to Choose ERCP
- Bile duct stones are confirmed and require extraction
- Biliary or pancreatic stenting is needed
- Sphincterotomy is indicated
- Post-surgical bile duct leaks must be repaired
- Therapeutic intervention and diagnosis are both needed in the same session
The EUS-First Strategy
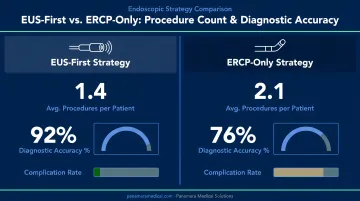
When the decision between EUS and ERCP isn't clear-cut, the evidence consistently favors leading with EUS. Karakan et al.'s prospective randomized trial of 120 patients showed EUS sensitivity of 91% versus 75% for endoscopic retrograde cholangiography alone in intermediate-probability bile duct stone cases. For small stones under 4 mm, the gap was more pronounced: EUS sensitivity 90% vs. just 23% for ERC.
The intervention counts tell a parallel story. The EUS-first group required 83 total procedures compared to 98 in the ERC-only group — 15 fewer procedures with direct implications for complication rates.
The ASGE 2019 choledocholithiasis guideline formally recommends EUS or MRCP to confirm diagnosis in intermediate-risk patients before committing to ERCP. EUS has comparable accuracy to diagnostic ERCP for CBD stones and a significantly lower adverse event rate.
Practical Barriers
EUS requires a trained interventional endoscopist and a dedicated echoendoscope. In centers lacking that infrastructure, ERCP may remain the practical default even when EUS would be clinically preferable. For many facilities, addressing that infrastructure gap is as much an operational decision as a clinical one.
Conclusion
There's no universal winner here. EUS and ERCP are complementary — EUS excels at imaging and sampling; ERCP excels at treating and intervening. The best outcomes come from matching the right tool to the right indication by a team that actually has both available.
As gastroenterology practices expand their pancreatobiliary programs, access to well-maintained, current-generation echoendoscopes and duodenoscopes becomes a direct factor in procedural quality.
Facilities looking to build or upgrade their EUS and ERCP capabilities — without absorbing the full capital cost of new equipment — can explore trade-in and buy-back programs through Panamera Medical Solutions, which sources and supplies pre-owned endoscopic equipment across North America, Europe, and South America.
Frequently Asked Questions
Why would a doctor order an endoscopic ultrasound (EUS)?
Doctors order EUS to evaluate unexplained abdominal symptoms, diagnose or stage pancreatic and GI cancers, characterize cysts, or obtain tissue biopsies. It's also commonly used when CT or MRI results are inconclusive and a clearer picture is needed before deciding on further intervention.
Will I be put to sleep for an endoscopic ultrasound (EUS)?
Most patients receive conscious sedation, meaning they stay comfortable and relaxed but remain responsive. Some centers use deeper sedation based on patient anxiety, body habitus, or procedure complexity.
Is ERCP considered high risk?
Yes, relative to most endoscopic procedures. Post-ERCP pancreatitis is the most common serious complication, affecting 3–10% of patients — and higher in those with suspected sphincter of Oddi dysfunction, prior post-ERCP pancreatitis, or difficult cannulation. Center volume and endoscopist experience play a significant role in outcomes.
How long do you stay in hospital after an ERCP?
Most uncomplicated ERCPs are outpatient procedures requiring 4–6 hours of post-procedure recovery before discharge. Patients who develop pancreatitis may require admission of 2–3 days for mild cases, up to 10+ days for severe complications.
Can EUS and ERCP be performed together in the same session?
Yes. In experienced centers, EUS is performed first to confirm findings, followed immediately by ERCP for treatment. This combined approach reduces total sedation exposure compared to scheduling the procedures separately.
Which procedure is more accurate for detecting pancreatic cancer?
EUS consistently shows higher sensitivity for detecting pancreatic masses, particularly small tumors under 2–3 cm, where sensitivity reaches up to 99% compared to 55% for CT — and it enables tissue sampling via FNA/FNB. ERCP is not a primary cancer detection tool but may reveal ductal changes that suggest malignancy.